IP Indian Journal of Clinical and Experimental Dermatology
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation
Author Details :
Volume : 5, Issue : 1, Year : 2019
Article Page : 24-29
https://doi.org/10.18231/2581-4729.2019.0006

Abstract
Introduction: Polymorphic light eruption (PLE) is the most common photodermatoses encountered in clinical practice. It is an idiopathic acquired disorder in which a delayed response to Ultraviolet radiation occurs in the form of skin eruptions consisting of papules, vesicles or plaques over the sun exposed and rarely on partially covered areas, distribution is generally symmetrical. Diagnosis is clinical and histopathological features vary according to age of lesions sampled.
Objective: To study clinical pattern and histopathological changes in patients with Polymorphic light eruptions in Malwa region (Ujjain, M.P).
Material and Methods: The present study is a hospital based observational study, conducted over a period of one year. A total of 100 cases including male and female patients presenting with history of photosensitivity or with clinical manifestations related to photosensitivity were enrolled. All patients underwent clinical and systemic examination followed by routine and histopathological investigations. The findings were recorded in proforma for analysis and interpretation of data.
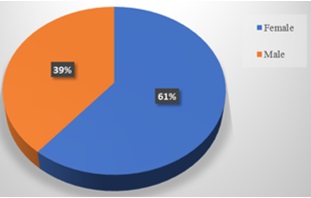
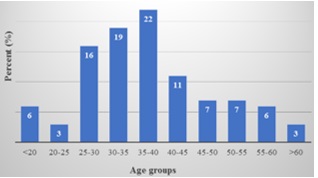
Results: In our study majority of patients were in the age group of 30 - 40 years (33%). PLE was more common in females (61%) compared to males (39%). The commonest lesion was papule then plaques but most of the patients had mixed presentation of various lesions. Most common site affected was neck followed by upper limbs. Histopathological findings were not very diagnostic, majority of the slides revealed spongiosis, parakeratosis and oedema of papillary dermis.
Conclusions: Diagnosis of PLE is clinical but still histopathology is required in doubtful cases to rule out other clinical differentials.
Keywords: Ple, Malwa region, Sun allergy, Clinicoepidemiology, Histopathology.
Polymorphic light eruption (PLE) often incorrectly referred as “sun allergy”. It is the most common type of photodermatitis. It is recurrent, acquired sunlight-induced immune mediated and of delayed onset disorder. The prevalence of PMLE varies from 10 to 20% in various studies across the world.[1],[2],[3],[4],[5]It is commonly seen in African, African Americans.[5],[6],[7],[8] Chinese and Indian. Its prevalence in India is 0.56%.[3] Occurrence is more frequent at higher latitudes and altitudes.[9] It is common during spring or early summer. The severity increases as summer progresses and diminishes in winters. PMLE is generally observed in the first three decades of life. The mean age in females is 33 years whereas in males it is 35 years.[1] Females are more often affected than males.[2]The etiology is unknown and is believed to be multi factorial. It has a polygenic mode of inheritance.[1],[2] It has many clinical variants, characterised by itchy papules, plaques and scales over exposed parts of body sometimes it can involve partially covered areas also. Diagnosis is clinical and histopathological findings are non-specific. Histopathological findings vary as early lesions show mild spongiosis with focal lymphocytic exocytosis and sometimes mild to moderate superficial and deep perivascular, periadnexeal lymphohistiocytic inflammatory infiltrate.[10] Condition is mostly self resolving. Treatment is symptomatic and further management depends on severity of disease.
Table 1: Classification of photodermatosis.
|
Immunologically mediated |
Polymorphous light eruption Actinic prurigo Chronic actinic dermatitis Solar urticaria Hydroa vacciniforme |
|
Drug- and chemical-induced
|
Exogenous: phototoxicity and photoallergy Endogenous: cutaneous porphyrias |
|
Genodermatosis |
Xeroderma pigmentosa Others |
|
Photoaggravated conditions |
Psoriasis Eczema- Atopic, seborrhoeic, allergic contact Lichen planus Rosacea and facial telangiectasia others |
It was a prospective observational study undertaken to study clinicoepidemiology and significance of histopathology in polymorphic light eruptions in adults. We excluded patients aged less than 18years, photoaggravated dermatoses induced by drugs, chemicals and with genetic and metabolic disorders. A total of 100 cases with polymorphic light eruption attending Out Patient Department of Dermatology, Venereology and Leprosy at C.R. Gardi Hospital, attached to R.D. Gardi Medical College, Ujjain (Madhya Pradesh) of Malwa region within the period of one year were randomly recruited for present study. All patients enrolled were above 18 years of age. Informed written consent was taken for their inclusion in the study. Detailed history, general, systemic and dermatological examination was done. A pre- structured proforma was used to collect above information, which also included month, age of onset of symptoms, severity, nature, aggravating factors, constitutional symptoms, family, past and drug history, occupation, duration of exposure to sunlight, outdoor activities, type of clothing, usage of cosmetics, sunscreens and previous treatment. Patient was clinically examined under headings of skin type (Fitzpatrick skin phototype scale), type of lesion, size, shape, colour, site, symmetry, associated symptoms, aggravating and relieving factors. All routine investigations like complete blood count, random blood sugar, liver enzymes, urine analysis and biopsy were carried out in all the cases. Photopatch testing was not done. Punch biopsy of each and every patient was done to find significant findings. (We aimed to study clinicoepidemiological and histopathological aspect of PLE). Obtained data was compiled, tabulated, summarized and manual statistical analysis done. Prior approval for the study and the protocol was obtained from the ethical committee.
Results
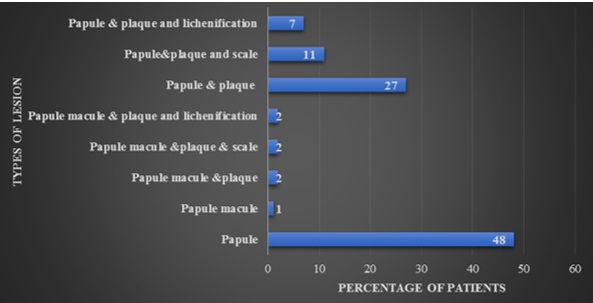
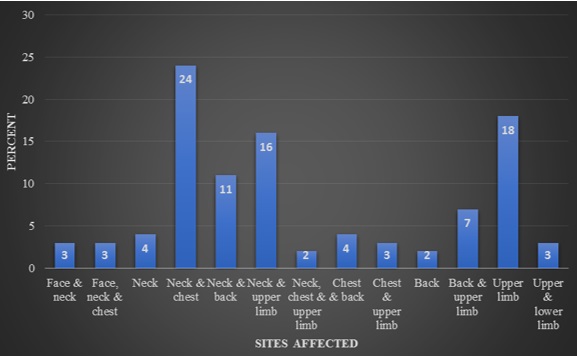
Prevalence of PLE calculated was 5% in Malwa region. Total 100 cases participated in the study, the minimum and maximum age were 18 and 66 years respectively. There were 61 females and 39 males with male to female ratio of 1:1.56. The majority of cases were found in the age group of 35-40 years (28%) followed by 30-35 years (19%). 71% cases were Hindus and only 19% Muslims were observed, reason for lesser prevalence in Muslims could be proper covering of the sun-exposed areas. Around 29% were illiterate patients, followed by who studied till high school (23%), middle school (21%), graduates & post graduates (16%) and then primary school (11%). In our study, maximum patients were farmers and labourers (38%) by occupation, while 18% were housewives. According to the Kuppuswamy classification, majority of cases belonged to the lower middle class i.e. 56% patients. Only 8% had family history of PLE. In the conducted study, 45% cases had skin type IV, 29% type V and type III (26%). Duration of disease in maximum cases was in between one to two months (36%), 32% patient had less than one month of duration. Majority of patients reported to us in late winters during the months of late January to early March (44%) and 33% in early summers. Maximum prevalence during late winters can be attributed to sun-bathing which is quite frequently practised in India. Most common type of lesion observed was papular i.e. 48%, followed by mixed presentation of papules and plaques in 27% of cases. Only 5 cases had macular eruption that too was mixed picture. 24% patients had lesions over neck and ‘V’ area of chest, 18% over extensor aspect of upper limbs. In most of the cases multiple sites were involved, generally over exposed parts but unexposed parts were also affected in few cases. 67% patients had lesions associated with itching, 21% were asymptomatic and remaining had burning sensation. Almost 52% of total cases had given the history of recurrence, transient in 20% and persistent in remaining. Biopsy was done in all the 100 cases. On histopathology examination, majority of slides 42% revealed spongiosis, oedema of papillary dermis and dense perivascular lymphocytic infiltrate in upper and mid dermis. These findings are characteristic of polymorphic light eruption. 18% of histology samples showed hyperkeratosis, oedema of papillary dermis and dense perivascular lymphocytic infiltrate in upper and mid dermis while few samples showed non-specific features.
 |
Click here to view |
Graph 1: Distribution of cases according to sex
 |
Click here to view |
Graph 2: Distribution of cases according to Age
 |
Click here to view |
Graph 3: Distribution of cases according to types of lesion
 |
Click here to view |
Graph 4: Distribution of cases according sites affected
Table 2: Distribution of cases according to skin types
|
Types of skin type |
Colour |
No. of patients (N) |
Percent (%) |
|
Type I |
Ivory |
0 |
0 |
|
Type II |
Beige |
0 |
0 |
|
Type III |
Medium brown |
26 |
26 |
|
Type IV |
Dark brown |
45 |
45 |
|
Type V |
Very dark brown |
29 |
29 |
|
Total |
|
100 |
100 |
Table 3: Distribution of cases according to Duration
|
Duration (in months) |
No. of Patients |
Percent (%) |
|
<1month> |
32 |
32 |
|
1-2months |
41 |
41 |
|
2-3months |
18 |
18 |
|
3-4months |
5 |
5 |
|
4-5months |
2 |
2 |
|
5-6months |
0 |
0 |
|
>6months |
2 |
2 |
|
Total |
100 |
100.0 |
Table 4: Distribution of cases according to histopathological findings
|
Histopathology |
No. of patients (N) |
Percent (%) |
|
1, 4, 5 |
42 |
42 |
|
1, 3, 4, 5 |
4 |
4 |
|
1, 4, 5, 6 |
5 |
5 |
|
1, 5 |
10 |
10 |
|
1, 5, 6 |
3 |
3 |
|
2, 4, 5 |
18 |
18 |
|
2, 4, 5, 6 |
4 |
4 |
|
2, 5 |
10 |
10 |
|
2, 5, 6 |
4 |
4 |
|
Total |
100 |
100.0 |
Keywords: 1 Spongiosis, 2- Hyperkeratosis, 3- Focal lymphocyte exocytosis, 4- Oedema of papillary dermis, 5- Dense perivascular lymphocytic infiltrate is present in upper and mid dermis, 6- Hydropic degeneration of basal cells.
Some Clinical and Histopathological images of patients studied.
 |
Click here to view |
Fig. 1: showing discrete papules and plaques over back of nec
 |
Click here to view |
Fig. 2: Maculopapular lesions present over back.
 |
Click here to view |
Fig. 3: Showing lichenified plaque over extensor aspect of forearm.
 |
Click here to view |
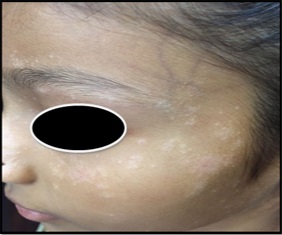
Fig. 4: Multiple macules and papules are present over face.
 |
Click here to view |
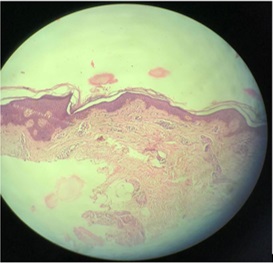
Fig. 5: Histopathology slide showing mild spongiosis and focal interface change.
 |
Click here to view |
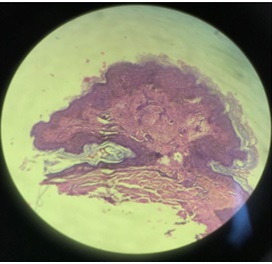
Fig. 6: Histopathological slide showing superficial and deep lymhocytic infiltrate.
Polymorphic light eruption being the most common type of photodermatosis. Its prevalence in India is 0.56%.[3] The present study was done in Ujjain district of Malwa region in Madhya Pradesh which is at a latitude of 23°09’ N and longitude of 75°43’ E. Tropic of cancer passes through Ujjain, here weather experience two distinct seasons of extreme hot summers and winters. People living in this region are in continuous exposure to sun and its rays. Prevalence of PLE calculated is 5% in Malwa region.
We included 100 cases, which showed female predominance, similar to other studies.[11],[12],[13],[14],[15],[16]In our study, maximum patients were farmers and labourers constituting 38% as major population of Malwa region comprise of farmers, followed by housewives (16%) and students (12%) similarly Chacko E et al in 2017 also showed maximum prevalence in farmers (29%).[8]. While other studies showed higher incidence in housewives.[13],[14],[15],[16]As per Fitzpatrick classification of skin type, type IV (dark brown) showed maximum prevalence (45%) of PLE, followed by type V (very dark brown) 29% then type III (medium brown) 26% in our study. Our results corresponded with a study conducted by Baliah K et al.[13] Majority of patients reported to us in late winters during the months of late January to early March (44%) and 33% in early summers. Sharma D et al in their study got highest prevalence (76%) in summers while just 24% in winters.[11] Sharma L et al in 2008 recorded 20.9% of prevalence in the month of March similar to our study and 15% in the month of September.[16] Maximum prevalence during late winters can be attributed to sun-bathing which is quite frequently practised in India. We observed papular eruptions as the most common lesions in 48% cases followed by mixed presentation of papules and plaques (27%), which corresponded with other studies. In our study majority of the patients showed involvement of two or more sites of which neck and ‘V’ area of the chest were commonest comprising 24%, followed by forearms (18%). It was also observed that if single area was involved, then neck was found to be more affected then forearms in more than 50% of cases. Some studies also favoured this observation while others reported forearms as the most common site affected. 52% cases showed recurrence of disease similar to Chacko et al.[12] In our study, majority of histopathology slides revealed spongiosis, oedema of papillary dermis and dense perivascular lymphocytic infiltrate in upper and mid dermis comprising of 42%, but similar findings can be seen in lupus erythematosus, eczema, lichen planus and few others. Similar to our study, Sharma D et al also found spongiosis, oedema of papillary dermis and lymphocytic infiltrate in 32.95% slides.[11] while Baliah K et al revealed hyperkeratosis, acanthosis and deep perivascular lymphocytic infiltrate as the most common finding.[13]
Conclusion
Polymorphic light eruption is the most common photodermatoses in Indian scenario. Its prevalence in Malwa region is 5%. A slight female gender predominance (61%) and adult age of presentation (30-40years) is a consistent finding in our study. Patients are mainly farmers and labourers by occupation. Majority had Type IV skin type. Pruritus was the most common symptom observed. The commonest lesions observed were papular seen over the neck and ‘V’ area of chest. Polymorphism in the clinical lesions is typical. Histopathological findings were specific but not diagnostic. Diagnosis is usually based on the clinical signs and symptoms, histopathology can be done in atypical cases. Recurrence is the rule if protective measures are not taken. Proper information regarding the disease and appropriate precautionary measures to be taken will help in reducing the incidence of disease.
Conflict of Interest: None.
How to cite : Verma K, Rokde R, Singh U, A clinicoepidemiological and histo-Pathological study of polymorphic light eruptions in malwa region. IP Indian J Clin Exp Dermatol 2019;5(1):24-29
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 4833
PDF Downloaded: 629