IP Indian Journal of Clinical and Experimental Dermatology
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation
Author Details :
Volume : 5, Issue : 1, Year : 2019
Article Page : 95-97
https://doi.org/10.18231/2581-4729.2019.0021

Abstract
Intoduction: Eccrine angiomatous hamartoma (EAH) is an extremely rare and benign malformation in adults which presents with single or multiple nodules or single large plaque over the extremities at birth with pain and marked sweating. On histopathological examination,there is increased proliferation of eccrine sweat glands and capillary vessels in the dermis. Herein we report a 43 year-old male who presented with a single hyperpigmented plaque over the hypothenar eminence of right palm associated with excessive sweating for 3 months duration.Biopsy from the lesion was suggestive of eccrine angiomatous hamartoma.This case has been reported due to it’s unusual adult onset.
Keywords: Eccrine angiomatous hamartoma, EAH, Benign tumor, Adult onset.
A 43 year old male, working as a supervisor in a hotel came with complaints of hyperpigmented plaque over right palm for 3 months duration which started as a small red itchy plaque. It was associated with excessive sweating over the plaque and pain following local pressure and physical exertion. No history of trauma or similar lesions in other parts of the body. No history of atopy. No history of hypopigmented patches or altered sensations over the extremities.
A solitary, well defined, hyperpigmented plaque of 5x3cm size present over the hypothenar eminence of Right palm. Plaque was tender, firm, cold, and incompressible with intact sensation. Amputated index finger following trauma on the left hand as shown in figure 1(b). Hair, nail, oral mucosa, genitals were normal and systemic examination was also normal.Clinical differential diagnosis were Glomus tumor,Tufted angioma, Blue bleb rubber nevus, Eccrine nevus, Hansen’s disease(due to amputated finger).
 |
Click here to view |
Fig. 1: a. hyperpigmented plaque on the right (blue arrow).
 |
Click here to view |
Fig. 1: b. Comparison with the normal left hand(note the amputated index finger on the left).
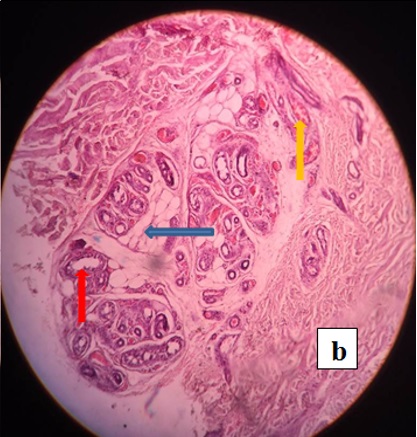
Routine investigations including Complete hemogram, Peripheral smear, Liver function test, Renal function test, ECG, Chest x-ray were normal. Ultrasound showed subcutaneous soft tissue thickening with no evidence of increased vascularity. Biopsy for HPE taken from the skin lesion showed hyperkeratosis, acanthosis, and increased in number of eccrine glands in mid and lower dermis with surrounding fat lobules, and stroma with abundant capillary angiomatous foci.Based on the clinical and skin biopsy findings, a diagnosis of Eccrine Angiomatous Hamartoma (EAH) was made and consequently surgical excision was planned but the patient was lost for follow up.
 |
Click here to view |
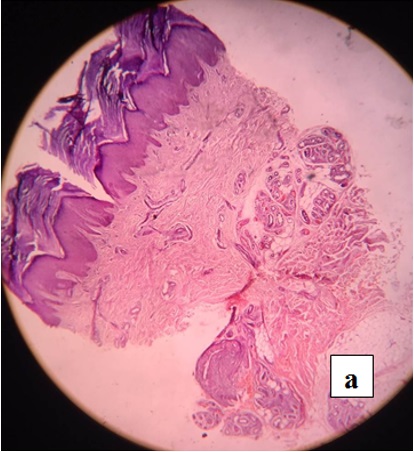
Fig. 2: a. Epidermis showing hyperkeratosis and acanthosis. Dermis showing increased no. of eccrine glands and capillaries.
 |
Click here to view |
Eccrine angiomatous hamartoma (EAH) is a benign and very rare cutaneous malformation usually appearing as a single macule or dusky bluish nodule or solitary plaque at birth or early in childhood although in our case it appeared at middle age. It can occur as multiple lesions sometimes. The size of the lesions varies from 2 mm to 3 mm to several centimeters. About 50 cases have been reported so far worldwide, out of which we could find only 8 cases in which the onset was during adulthood, as in our case.[3] The lesions may mostly favour extremities where there is increased number of eccrine glands mainly in palms and soles associated with pain or tenderness and hyperhidrosis.[4],[5],[6]Pain is seen in 42% and hyperhidrosis in 32 % of the cases.[2] Uncommon variants of EAH are verrucous EAH where it resembles angiokeratoma or verrucous hemangioma, and palmar cutaneous hamartoma where in addition to fats, capillary channels and eccrine glands, there is neurovascular glomic bodies.[4],[2]On HPE, Eccrine angiomatous hamartoma shows multiple dilated secretory and ductal parts of eccrine glands that are surrounded by capillary vessels and lymphatic channels in deeper dermis with invasion of adipose fats, nerve fibers, hair follicles and mucin sometimes.[4],[6]Tenderness of the lesions may be due to presence of small nerve branches in between the eccrine ducts. The exact etiology of EAH is unknown but it has been proposed that there is a faulty in differentiating epithelial-mesenchymal interactions leading to excessive proliferations of eccrine glands and vessels or due to faulty induction of heterotypic dependency during organogenesis.? Late onset EAH can be due to recurrent trauma but in our case the patient denies any history of trauma. Neurofibromatosis type 1 has also been reported with EAH. Starch-iodine test can be done to demonstrate hyperhidrosis. Common clinical differential diagnosis includes Eccrine nevus, Eccrine poroma, tufted angioma, Glomus tumor, Blue bleb rubber nevus which can be easily differentiated by specific histopathological findings. Eccrine nevus can present clinically as a well circumscribed area of hyperhidrosis with a sweat discharging pore or papular lesions arranged in linear fashion and histologically distinguished by increase in number and size of eccrine coils without increase in capillary channels and fatty tissues.?3; Eccrine poroma usually presents with asymptomatic skin colored nodular lesions on palms and soles with nests of small keratinocytes attached to epidermis, the number and size of eccrine glands, capillary channels are usually normal in eccrine poroma. Tufted angioma is also a close differential as it can present with hyperhidrosis but histopathologically there is proliferation of all the dermal capillaries giving cannon ball appearance. Glomus tumors can also present at third or fourth decade as single small bluish red nodule on the palms, subungual region of fingers and foot associated with pain on exposure to cold or pressure and histologically glomus cells surrounds vascular spaces with rows of round dark nuclei and little cytoplasm giving the appearance of string of black pearls.[5],[7]A blue rubber bleb nevus can present at birth a s soft, dark blue nodules with irregular spaces in the lower dermis with RBCs and fibrinous materials on HPE. Generally speaking, aggressive treatment is unwarranted in EAH since it is usually benign and slow growing. Botulinum toxin injection and aluminum chloride can be tried for hyperhidrosis. Surgical excision, Lasers and Sclerosants are other treatment options in symptomatic and cosmetically disfiguring patients. Surgical excision is usually curative in selected patients. Very rarely amputation of acral parts are indicated in extensive lesions.? Spontaneous regression has been reported in some cases.?2;
This case is reported due to its rarity and unusual adult onset.
How to cite : Khro N, Revathy M, A case report of adult onset eccrine angiomatous hamartoma: A rare entity. IP Indian J Clin Exp Dermatol 2019;5(1):95-97
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 3185
PDF Downloaded: 509