Introduction
Capillaroscopy is an investigational tool to examine microvascular changes and is often performed in patients with different diseases associated with abnormal microcirculation.1 The reasons for performing this procedure may be to understand pathophysiology, rule out some diseases, evaluate disease progression, start new treatment and/or to monitor the response to therapy.2, 3, 4 The procedure is useful in several diseases, especially in Raynaud phenomenon and some autoimmune diseases. 5 Capillaroscopy can also be an important investigational tool to detect microvascular changes in patients with scleroderma-spectrum disorders. 3
Nail fold capillaroscopy is an easy imaging method for early diagnosis, qualitative and quantitative examination and analysis of structural changes in capillaries present in the nailfold.6, 7 Simple procedure, non-invasive tool for analysis of microcirculation and safety are the advantages of this method. 3, 5, 8, 9, 10 It can be done in both children as well as adult patients. 5 Involvement of nail fold capillaries in the early course of disease process is known in patients with connective tissue disorders. Different abnormalities of microcirculation including dilated capillaries, capillary dropouts and splinter hemorrhage are commonly observed on nail fold capillaroscopy is patients with connective tissue diseases. Capillaroscopy can be useful tool for forecasting the risk of visceral complication and digital ulcers in systemic sclerosis. 7 Other applications of nail-fold capillaroscopy include differential diagnosis of digital necrosis and diffuse interstitial lung disease.
With the above mentioned practical uses and benefits, nail fold capillaroscopy is gaining importance day by day especially in rheumatology and dermatology practice for early diagnosis of connective tissue diseases. 7, 8, 9
Methods of performing nail fold capillaroscopy have evolved over the years. Nail fold video capillaroscopy is gold standard, but it has limitations including need for a special instrument and hence cost. It is also time-consuming and limited portability. Handheld dermoscope can overcome these limitations. 11, 12 Other options include use of magnifying lens, ophthalmoscope, dermatoscope, stereomicroscope and a wide field microscope.12
There is limited literature with small studies from India on the clinic-epidemiological characteristics of capillaroscopic changes in connective tissue disorders. 11, 12, 13, 14
Objective
The objective of this study was to evaluate nail changes in different collagen vascular diseases using the capillaroscopic technique.
Materials and Methods
In this prospective, observational study, consecutive patients of both gender diagnosed with collagen vascular diseases presenting to dermatology department of a tertiary care hospital were included. After detailed history and clinical examination, all enrolled patients were subjected to capillaroscopy of periungular nail of both hands. Hand dermatoscope (Veos HD2 canfield with IPhone 7) was used for performing capillaroscopy. Capillaroscopic findings were recorded in all enrolled patients. Presence of seven to 11 capillaries in a hairpin shape was considered as normal pattern. 5 Observed morphological and structural abnormalities in microvasculature in the nail bed in all patients were recorded and tabulated. Differences in the prevalence of capillaroscopic changes between connective tissue disorders were noted. The study was initiated only after obtaining approval from the Institutional Ethics Committee.
Statistical analysis
Descriptive statistics of collected data are presented in this paper. Continuous variables (i.e. age and duration of disease) are presented as mean and standard deviation. Categorical data i.e. demographic details other than age, prevalence of different connective tissue disorders and observed abnormalities) are presented as frequency and percentages.
Results
In this study, a total of 50 patients [females 43 (86%)] were enrolled. The mean (+SD) age of study participants was 38.20 (+10.51) years. The study included 25 (50%) housewives and 9 (18%) housemaids. The mean ± SD disease duration noted in our study was 1.96 ± 1.12 years, ranging from 6 months to 5 years (Table 1).
Patients with systemic sclerosis and systemic lupus erythematosus constituted 17(34%) and 16 (32%) patients respectively (Table 1). There were six (12%), five (10%) and three (6%) patients with discoid lupus erythematosus, dermatomyositis and mixed connective tissue disease respectively.
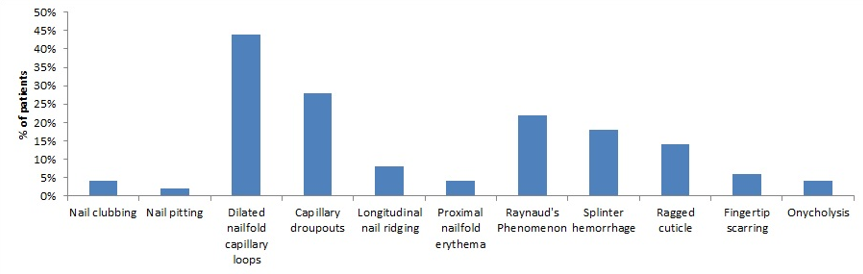
Nail clubbing was observed only in two (4%) patients. Both patients had discoid lupus erythematosis, constituting 33% of total patients with it. Only one patient had nail pitting. He had mixed connective tissue disorder. A total of 22(44%) patients had presence of dilated nailfold capillary loops/giant capillaries (Figure 1). Capillary dropouts, longitudinal nail ridging, proximal nail fold erythema, Raynaud’s phenomenon, splinter hemorrhage, ragged cuticle, fingertip scarring, and onycholysis among 14(28%), 4 (8%), 2(4%), 11(22%), 9(18%), 7(14%), 3(6%) and 2(4%) patients respectively (Figure 1).
Out of 17 patients with systemic sclerosis, 15(88.23%) showed presence of dilated nail fold capillary loops/giant capillaries whereas capillary drop-pouts were present in 14 (87.5%) patients.
howscapillaroscopic changes in patients with systemic sclerosis. A total of 15 (88.23%) patients with systemic sclerosis showed presence of dilated nail fold capillary loops or giant capillaries. Capillary dropouts were observed in 14 (82.35%) patients. Raynaud’s phenomenon, splinter hemorrhage and fingertip scarring was observed in 11(64.71%), 6(35.29%) and 33(17.65%) patients respectively (Table 2). Longitudinal nail ridging, ragged cuticle and onycholysis was observed in one patient each.
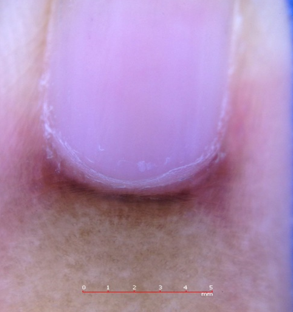
Capillaroscopic changes observed in patients with systemic lupus erytematosus are listed in table 3. Ragged cuticle was observed in four (25%) patients with systemic lupus erythematosus (Figure 2).
Dilated nailfold capillary loops, splinter hemorrhage (Figure 3) and proximal nail fold erythema (Figure 4) were observed in two (12.5%) patients each (Table 3). Longitudinal nail ridging and onycholysis was seen in one patient each.
A total of five patients in the study had dermatomyositis of whom three (60%) showed presence of dilated nail fold capillary loops/giant capillaries. Splinter hemorrhage and ragged cuticle were seen in one (20%) patients each. Out of six patients with discoid lupus erythematosis, 2(33.33%) had presence of longitudinal nail ridging and one (16.67%) had ragged cuticle. Out of three patients with mixed connective tissue disorder, two (66.67%) showed dilated nail fold capillary loops/giant capillaries.
Table 1
Baseline characteristics of study participants
Table 2
Capillaroscopic changes in patients with systemic sclerosis (n=17)
Table 3
Capillaroscopic changes in patients with systemic lupus erythematosus (n=16)


Discussion
Collagen vascular disorders are associated with microangiopathic alterations in nail folds 11 and capillaroscopy is gaining popularity as a non-invasive procedure having diagnostic and prognostic usefulness in patients with connective tissue disorders. 5 Raynaud's phenomenon is one of the important indications for performing nail fold capillaroscopy. 2
In this study, we examined capillary changes in nail bed of 50 adult patients with connective tissue disorder. In our study, mean age of patients was lower than another study. This could be due to the type of patients included in the study. Patients in our study were walk in patients with connective tissue disorder whereas in another study were referred patients who are usually with prolonged illness. 15
Females significantly outnumbered male population in our study. Similar higher involvement in females is also reported by others. 15, 16 Housewives and housemaids constituted 50% and 18% of overall population in our study.
Systemic sclerosis and systemic lupus erythematosus were the two most common connective tissue diseases constituting about two third of our study population. Our observations are in line with another study (n=30) from Amritsar (India) which evaluated changes in collagen vascular disorders by dermoscopy. The authors reported 53.3% and 36.7% patients with systemic sclerosis and systemic lupus erythematosus respectively. 11 In our study, prevalence of systemic sclerosis was only slightly more than that of systemic lupus erythematosus.
In our study, overall, the most common finding was dilated nail fold capillary loops/giant capillaries. Second commonest finding was capillary dropouts. Another small study from India also reported similar observations. However, the prevalence of dilated capillaries and capillary dropouts in our study was lower than reported in a study. 11
Although the importance of early diagnosis and management of systemic sclerosis is well understood, detection at very early stage may not be easy when there is absence of typical clinical features. Capillaroscopy has a known significant role in the diagnosis of systemic sclerosis. 3
Capillaroscopic changes are common in systemic sclerosis and these patients have specific and early changes. Due to this reason capillaroscoy has high potential for detecting disease at very early stage. 2, 3, 8 Raynaud's phenomenon and microvascular changes may be some of the early signs of systemic sclerosis. 17 Giant capillaries and microhaemorrhages on nail fold videocapillaroscopy is hallmark of early scleroderma. 18 Capillaroscopy has also been involved in the classification criteria for systemic sclerosis. 3
A study reported typical scleroderma capillary pattern i.e. megacapillaries and reduced capillary density in 87.5% and 61.6% patients with diffuse and limited cutaneous systemic sclerosis respectively. 19 In our study also, most of the patients with systemic sclerosis showed presence of dilated capillaries. Capillary dropout was the second most common observation in patients with systemic sclerosis. Raynaud’s phenomenon and splinter were also seen in many patients with systemic sclerosis. Longitudinal nail ridging, ragged cuticle and onycholysis were observed only in one patient each. Observation of systemic sclerosis pattern on nail capillary microscopy is common in patients with Raynaud's phenomenon, and in those with connective tissue diseases other than systemic sclerosis. 1
A comparative study showed more common nailfold capillaroscopic abnormalities in patients with systemic lupus erythematosus as compared to controls. 20 Specificity of capillaroscopy changes has also been reported to be high.21In our study, ragged cuticle was most common abnormality in patients with systemic lupus erythematosus. Other abnormalities in patients with systemic lupus erythematosus included dilated nail fold capillary loops, splinter hemorrhage and proximal nail fold erythema. Longitudinal nail ridging and onycholysis were observed in one patient each. Scleroderma pattern has been reported to have higher risk of pulmonary arterial hypertension in patients with systemic lupus erythematosus. 21 These findings suggest that patients with systemic lupus erythematosis can be screened with nail fold capillaroscopy to identify high risk patients for this complication.
Nail capillaroscopy in mixed connective tissue disorder may be a useful indicator to understand likehood of lung involvement and disease severity. 22 Presence of giant capillaries can suggest presence of interstitial lung disease in these patients. 23 In our study, there were only three patients with mixed connective tissue disorder. In two of these patients, dilated nail fold capillary loops were observed.
Another study also reported high specificity for nail capillaroscopy patterns in polymyositis/dermatomyositis. 24 The results of a large study showed that capillary microscopy can differentiate primary from secondary Raynaud's phenomenon. It can be useful for prediction of scleroderma spectrum disorders in patients with Raynaud's phenomenon. 16
Although nail bed changes are common in connective tissue diseases, they should be differentiated from other diseases such as due to diabetes mellitus or paraneoplastic syndromes. 8
Single center study and small sample size are the limitations of our study. Considering these limitations, our observations cannot be generalized. Larger multi-center studies are necessary to confirm our observations.
Conclusion
Systemic sclerosis and systemic lupus erythematosus were two most common connective tissue disorders in our study population. Dilated nail fold capillary loops/giant capillaries was the most common finding in overall population Dilated nail fold capillary loops, capillary dropouts, Raynaud’s phenomenon, splinter hemorrhage and fingertip scarring were common findings in patients with systemic sclerosis. Ragged cuticle was the commonest observation on capillaroscopy in patients with systemic lupus erythematosus. Overall, we found that capillaroscopy, a non-invasive is safe investigational tool in patients with connective tissue disorders.