Introduction
A 40-year-old female presented with a solitary lesion on the face since last six to seven years. On enquiry, the patient revealed that it was asymptomatic and non-progressive. Local skin examination demonstrated a single, dome-shaped, skin coloured nodule with fine hair jutting out from a central pore at its summit [Figure I]. The lesion was non-tender and firm inconsistency and the hair on its top could be epilated easily with plain forceps. Surrounding skin showed multiple flat warts and dermatosis papulosa nigra. On systemic examination, no abnormality was identified. A clinical impression of benign adnexal neoplasm probably solitary trichoepithelioma or a trichofolliculoma and giant molluscum was kept, and the patient was advised excisional biopsy which would also be curative in this case.
Histology of the biopsy specimen revealed a fairly well-circumscribed neoplasm comprising of a large dilated cystic cavity lined with squamous epithelium differentiating towards follicular infundibulum and containing keratin. Multiple small immature and abortive hair follicles were seen radiating from the primary hair follicle in a stroma rich in fibroblasts [Figure-II, III]. Few epithelial strands are seen interconnecting the secondary hair follicles. These findings confirmed our clinical impression of a trichofolliculoma. No recurrence has been noted till date following the excision.

Figure 2
Multiple small immature and abortive hair follicles were seen radiating from the primary hair follicle (Scanner View – 4x)
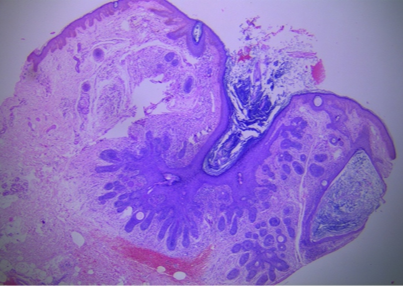
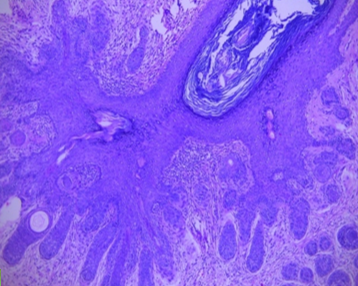
Figure 3
Multiple small immature and abortive hair follicles were seen radiating from the primary hair follicle (High Power – 10x)
Trichofolliculoma is a rare benign adnexal neoplasm with follicular differentiation first described by Miescher in 1944.1 Usual presentation is of a solitary skin coloured, dome-shaped papule or nodule with a tuft of vellus hair jutting out from a central dell. It is predominantly seen in adults in the head and neck region. Childhood-onset is rare. Presence of tuft of vellus hair arising out of the lesion is a distinctive clinical sign of this lesion which made clinical diagnosis easier in our case too. Characteristic histopathology of a central dilated cystic cavity lined by squamous epithelium with a well-formed granular layer and keratin as its content resembling infundibulum of a hair follicle and secondary follicles radiating from its wall differentiates it from other histological mimickers like trichoepitheliomas. Two variants of trichofolliculomas include sebaceous trichofolliculoma and folliculo-sebaceous cystic hamartoma that may represent an evolutionary stage. 2, 3
Histologically trichofolliculoma has been categorized into 3 stages- early, fully developed, and late stage. In Early-stage, trichofolliculoma is small in size, superficial in location and composed of several vellus hair follicles in the anagen phase, projecting to an infundibulum. In Fully-developed stage, trichofolliculomas demonstrate a central infundibular cyst, in this stage multiple vellus hair follicles in anagen phase arising from its follicles in this stage are without any sebaceous differentiation. Late-stage trichofolliculoma is characterized by an infundibular cyst with multiple malformed vellus hair follicles and sebaceous differentiation. A prominent stroma is present with many dilated vessels, numerous fibrocytes, as well as fibrillary bundles of collagen perifollicular sheath thickening is progressively increased from early to late-stage and in late-stage sometimes it may be associated with mucinosis and adipose tissue.4
The classical trichofolliculoma does not have sebaceous acini; however sebaceous trichofolliculoma variant shows abundant sebaceous acini.
On immunohistochemistry, trichofolliculoma demonstrates positivity for cytokeratin 14,15,16,17 which is useful to differentiate it from other benign tumours.4
Another useful aid to the diagnosis of trichofolliculoma is dermatoscopy showing peripheral radial dark brown projections resembling a crown and described as ‘firework pattern’. These projections represent the nests of cells radiating from the follicular epithelium.5
These are benign hamartoma and do not have any systemic complications. Various therapeutic options are- Laser Ablation, Deep shave removal, Punch excision, Excisional surgery, Electrosurgery, but the treatment of choice will be simple surgical excision.
We report this case for its rarity of occurrence, and clinical resemblance to solitary trichoepithelioma.