Introduction
Dermato-epidemiology is an important emerging scientific discipline that investigates the distribution and determinants of skin disease in specified populations. 1
The burden of skin and subcutaneous diseases measured in DALYs was 42,883,695.48 (95% UI, 28,626,691.71-63,438,210.22) in 2019, 5.26% of which were years of life lost and 94.74% of which were years lived with disability. The highest number of new cases and deaths due to skin and subcutaneous diseases were recorded in South Asia (new cases, 25%; deaths, 25%), and, especially in India (new cases, 19%; deaths, 25%). 2
Although mortality due to skin diseases is low, they contribute to significant morbidity, disability and social stigma which is a significant health concern having more psychological and physical impact than that due to cardiovascular diseases in India. In the global burden of disease study 2017, skin diseases ranked 10th whereas cardiovascular diseases ranked 12th according to age-standardised years lived with disability. 3
Skin is considered as the mirror of internal organs and serves as a window to various latent internal diseases. Early identification of skin disease is important not only for treating patients but for preventing the spread of communicable diseases.
Skin diseases have varied prevalence in different regions according to the racial, genetic, environmental, and socio-economic conditions.4 Eczematous dermatoses are common in developed countries whereas infections and infestations are common in developing countries because of malnutrition, overcrowding, inadequate hygiene and lack of awareness. In developing countries, it was reported 70% of people suffer from skin disease at some point of their lives. The prevalence of skin diseases in India among the general population has varied from 6.3% to 11.2% in various studies. 5
Researches to determine the pattern of skin diseases are very important for proper health care planning and management. This suggests a methodology for the practice of community dermatology, a subject relatively untouched in the literature.
Although there is adequate literature on the pattern of skin diseases in the general global population, there is a paucity of such work in developing countries. Most epidemiological information about skin diseases we possess is from hospital-based studies. They may not actually represent the real prevalence of skin disease in the community as compared to community level medical camps.
In this study we report the pattern of skin diseases observed in population who attended various rural health camps conducted in Pudukottai district of Tamil Nadu. Direct outreach to the community like the present one is more likely to yield a more closely representative data. This study provides a valuable insight into epidemiologic parameters like the pattern of skin diseases in the community, the age groups affected, the gender prevalence, and the relative lack of knowledge about the need to seek dermatological intervention. The data provide us an insight into the dermatological conditions in the community and the need for initiating interventions in the community to make them aware about the common dermatological conditions.
Materials and Methods
This study was executed after obtaining approval from Institutional Ethics Committee, Karpaga Vinayaga Institute of Medical Sciences and Research Centre, Chengalpattu, Tamil Nadu, India. This is a community based, cross sectional study in which the cases attending the rural preventive medical camps, conducted in the rural communities of Pudukottai district of Tamil Nadu, India were included in the study. All the patients attending the camps were included in the study among which patients with dermatological complaints were screened separately and detailed history obtained and examined clinically. The study was divided into following parts: Selection of the study population, history taking and data collection, clinical examination, and diagnosis.
Inclusion criteria
All newly diagnosed cases presenting with skin diseases, all ages and both sexes, with parent and/or guardian giving consent for the participation in this study.
Exclusion criteria
Patients not willing to give consent to participate in the study. Cases with incognito diagnosis and those that need exhaustive investigative work up for confirming the diagnosis were also excluded from the study.
A brief relevant clinical history was elicited, with the use of a preformed questionnaire. The variables in this questionnaire included demographic variables (age, gender, place, or residence); socioeconomic variables (education, occupation); and self-reported history of comorbidities. History of smoking tobacco, alcohol consumption and family history of skin diseases were also included. Physical examination was carried out by standard methods including Outpatient based confirmatory tests like woods lamp examination, KOH mount etc. and vitals were recorded. A thorough dermatological examination was performed. Instruments used in this study were magnifying lens, Derma lite DL4 dermo scope, woods lamp, measuring tape, torch and disposable gloves to aid in the diagnosis.
The diagnosis was entirely based on clinical assessment of the dermatologists at the field, and no major dermatological investigations like biopsy were conducted due to the unavailability of investigative facilities in the rural medical camp setup. Those cases requiring specialized investigations for aiding diagnosis were referred to the Department of Dermatology, Karpaga vinayaga institute of medical sciences and research centre, Chengalpattu and were excluded from the study.
Data collected were compiled based on age, sex, prevalence of dermatoses, and pattern of dermatoses. The data was analysed and manuscript prepared in Microsoft word 2017 version. We compared means with t-test, medians with Mann–Whitney test, and proportions with Chi-square test. A level of P < 0.05 was used to indicate statistical significance in all analysis.
According to aetiology, all the skin diseases were classified into two groups, viz. infective and noninfective diseases.
The infective dermatoses were further grouped as
Bacterial infections (folliculitis, impetigo, erythrasma, pitted keratolysis, mycobacterial infections)
Fungal infections (dermatophytosis, candidal infections, onychomycosis, pityriasis versicolor)
Viral infections (herpes simplex, herpes zoster, verruca)
Arthropod infections (scabies, pediculosis, elephantiasis)
The noninfective dermatoses are further classified as
Appendageal disorders (acne vulgaris, miliaria/ sweat dermatitis, telogen effluvium, alopecia, palmoplantar hyperhidrosis)
Benign skin tumours (syringoma, seborrheic keratoses)
Collagen skin disorders (keloid, morphoea, post traumatic scar, contractures)
Drug reaction (fixed drug eruption, drug induced pruritus)
Eczema (allergic/ irritant contact dermatitis, photodermatitis, atopic eczema, seborrheic dermatitis, stasis eczema, pityriasis alba, etc)
Geno dermatoses (nevi, angiokeratoma)
Metabolic skin disorders (acanthosis nigricans, diabetic dermopathy, nutritional dermatoses, uremic pruritus)
Neurodermatitis (prurigo simplex, prurigo nodularis)
Papulosquamous disorders (psoriasis, lichen planus, pityriasis rubra pilaris)
Pigmentary dermatoses (vitiligo, melasma, post inflammatory hypo/hyper pigmentation, Riehl’s melanosis, facial melanosis)
Vascular disorders of skin (acute/ chronic urticaria, cherry angioma, vasculitis)
Results
A total of 5870 patients attended the multi-speciality rural health camps conducted in the Pudukottai district over a period of 3 months from August 2023 to October 2023. Of these, 1456 (25%) patients had dermatological complaints. In our study, Males constituted 57.2% of the study population (n-833) and females constituted 42.8% (n-623). The most common age group affected is 41- 60 years 40.9% (n-596), followed by 21- 40 years 30.8% (n- 448), <20 years – constitute 17.7% (n-258) and > 60year age group 10.6% (n-154). The mean age of the study population is 38.8years. The common occupation encountered in our study population were students, farmers, followed by housewives and manual labourers.
Of the total number of dermatological cases (n-1456), infections contribute 31.6% of the cases (n-460), whereby non-infectious dermatoses seen in 68.4% of cases (n- 996).
Among the infectious conditions, fungal infections were the most common constituting 71.6% (n- 332), followed by bacterial infections constituting 12.1% (n-56), arthropod infections constitute 11.2% (n- 52), viral infections constitute the least accounting 5.2% (n- 24). Dermatophyte infections are the most common among fungal infections contributing 68.7% of the fungal infections and 34.3% of the total infectious cases and 15.5% of the total dermatological disorders. The five most common infections in the study group are Tinea corporis, followed by pyoderma, pityriasis versicolor, scabies and verruca vulgaris.
Fungal infections were seen most in 41-60 years, whereas bacterial, viral infections and arthropod infestations are more common in < 20years age group.
Among the non-infectious dermatoses (n- 996), eczema cases constitute 36.70% (n-366), followed by appendageal disorders 16.7% (n-166), pigmentary and vascular disorders each contributing 12.7% (n- 126 each), followed by neurodermatitis 5.6%, papulosquamous disorders contributing 4.4%. metabolic skin disorders seen in 3.2%, Benign skin tumours were seen in 2.8%, collagen disorders seen in 2.4%, drug reaction contribute 2.4%, Geno-dermatoses cases contribute 0.4%.
Among the eczematous disorders, allergic contact dermatitis (ACD) constitutes the most common form of eczema 26.1%, followed by photo-contact dermatitis, stasis eczema, miscellaneous eczema in 20.7%, 19.5%, 16.3%. Atopic eczema constitutes 5.4% of the eczema cases. Acne constitutes 40.5% of the appendageal disorders, followed by telogen effluvium and sweat dermatitis (26.2% each). Melasma contributes 62.5% of the pigmentary disorders and urticaria constitutes 90% of the vascular disorders. The most common non-infectious dermatoses in order are eczema, urticaria, melasma, acne and prurigo constituting 36.5%, 11.5%, 7.9%, 6.8% and 5.5%.
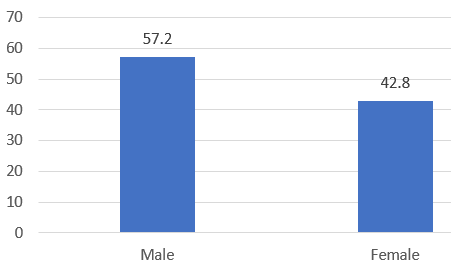
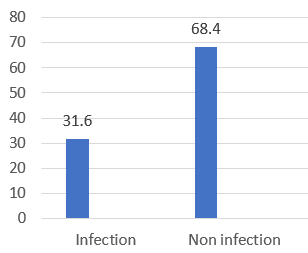
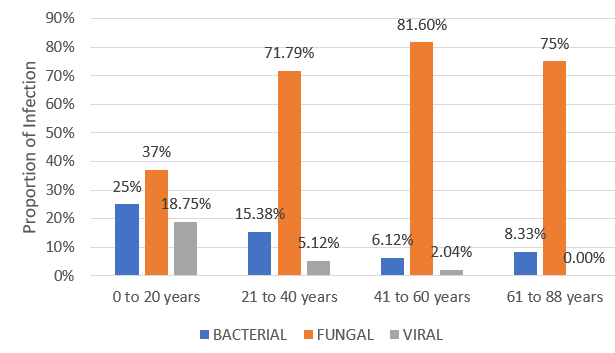
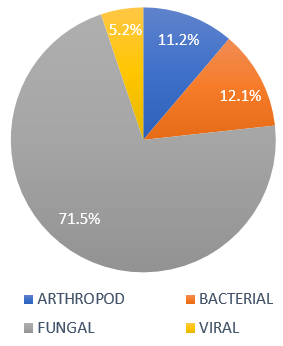
Table 1
Age distribution among non-infectious dermatoses
|
Age category |
n=cases |
% of Total |
|
1 to 20years |
195 |
19.5 % |
|
21 to 40years |
294 |
29.5 % |
|
41 to 60years |
399 |
40.2 % |
|
61 to 88years |
108 |
10.8 % |
|
Total |
996 |
100 % |
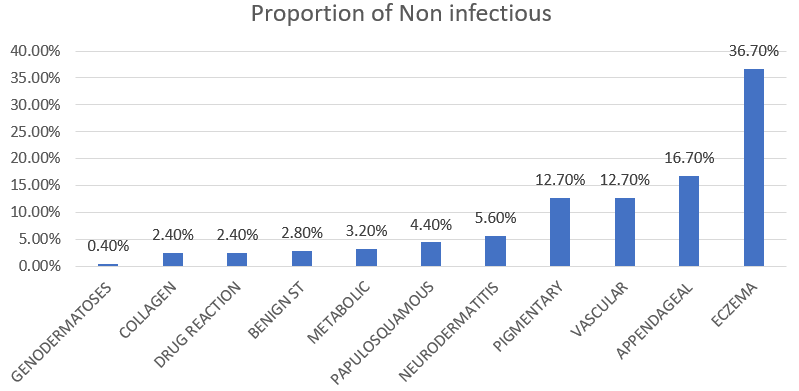
Table 2
Diagnosis vs Age group among Non-infectious dermatoses
Table 3
Sex distribution



Discussion
The prevalence of skin diseases in the general population in different geographic regions of India varies from 7.9% to 60%. 6 In our study, the proportion of dermatology cases contribute 12.50% of the general population. This percentage is like the study conducted by Asokan et al. 7 in which skin diseases contribute 10.55% of the total out patient cases of the hospital. This indirectly reflects the burden of skin disease in that population.
The most common age group in our study is 41-60 years. This age group constitutes the major proportion of the population in general. This age group constitutes the larger proportion of our population and they actively participate in community health checkups. This is similar to the study conducted by Manapurath et al. 8
Males outnumbered females in our study. This is similar to the study conducted by Bhuvnesh shah et al. 9 where males constitute 53% and females 47%. In our study it is attributed to the fact, males participate more in our study setting like rural camps.
The common occupation of our study group are students, farmer, housewives.
The common group of dermatological disorders in our study falls under non-infectious dermatoses (68.4%). This shows the changing trends in the prevalence of dermatological disorders and the increased exposure of patients to environmental pollution, increased cosmetic concerns regarding acne and pigmentary disorders. Most of the infectious dermatoses are of shorter duration and they will be treated by the primary health care physicians. This is similar to the study conducted by Uma devi et al. 10 where noninfectious dermatoses are seen in 68% of the dermatology OPD cases. Whereas in the study conducted by Kar et al. 11 infectious dermatoses constitute 57.8% of the OPD cases.
Among the non-infectious dermatoses, eczema (36.70%) is the most common condition we encounter. This is because of the increased use of pesticides, increased exposure to parthenium plants and exposure to detergents, etc. Acne cases contribute 16.7% of noninfectious dermatoses of our study and is more common in 20-40 years age group. This is because of the increased prevalence of acne in adolescent and adult age group and the increasing cosmetic concerns in this age group. Melasma contributes the highest proportion (12.7%) of pigmentary disorders and is more common in middle age females. This is attributed to various causes like hormonal, familial and increased sun exposure. These findings are consistent with the studies conducted by vinitha gupta et al. 12 where the top 3 noninfectious dermatoses were eczema, acne and urticaria. In the study conducted by Rao et al. eczema cases contribute 32.19% of the study population.
Infectious dermatoses constitutes 31.6% of our study population. Among these, the most common is fungal infections (71.6%) followed by bacterial (12.1%), arthropod infections (11.2%). Fungal infections constitute 22.6% of the total cases. In the study conducted by Bhargava S et al. 13 it is stated that fungal infections are seen in 20-25% of the population. This can be attributed by the fact that fungal infections are increasingly becoming chronic and antifungal resistance is also on the rise. Antifungal therapy needs longer duration of treatment and impose a financial burden to the patients. Many over the counter steroid drugs leads to increasing tinea incognito cases. On the other hand, pyoderma and scabies cases are more prevalent under 20 years age group. This can be due to malnutrition, overcrowding and unhygienic environment. There is also decreased immunity in these age group and the need for increased hygienic practices.14
Common diagnosis in relation to the gender are as follows: Eczema, fungal infections and appendageal disorders are seen more commonly in men whereas pigmentary disorders are more prevalent among females in our study.15
According to the age group, appendageal disorders are more prevalent among 21-40 years, pigmentary disorders in 40-60 years followed by 20-40 years. Neurodermatitis are seen more commonly above 60years of age in our study.
Conclusion
Our study depicts the pattern of dermatological diseases among the rural population in Tamil Nadu. Most of the prevalence studies available are hospital based and will not show the needs of the community. Our study is unique as there are few similar studies depicting the real prevalence of the dermatoses among the community rural population. Epidemiological studies help in formulating health policies and will reflect the original case burden of that area. The generalizability of the study has certain limitations as this is a cross sectional study and follow up of patients are not done. And the cases are diagnosed solely on clinical diagnosis without any confirmatory evidence as it a rural camp and facilities for confirmation are not available. Despite these limitations, this study will provide us a valuable insight into the real burdern of skin disorders in rural areas of Tamilnadu. Further research could explore specific conditions prevalent in each age group, contributing to a more detailed understanding of dermatological health. Promoting preventive measures and early detection can significantly impact the overall burden of dermatological conditions.