Introduction
Erythema nodosum leprosum.1 (ENL) is the common immunological complications of multibacillary leprosy. Classical lesions. 2, 3 of ENL are painful nodules and has systemically compromising symptoms. Eventhough these acute inflammatory episodes are common entity in the MBMDT treatment course, delayed recognition of the atypical presentations of ENL make the management exhausting due to development of complications.
ENL or type 2 reaction is the type III immunological reaction occuring mostly in lepromatous pole and classically characterized by crops of erythematous evanescent tender papules and plaques. Systemic involvement includes involvement of other organ systems like eyes.,4 testes.,5 nerves.,6 liver and kidney.7
Erythema nodosum leprosum is considered aberrant when present other than classical erythematous tender nodules. These aberrant presentations can present during the treatment of leprosy or present as a primary episode. Certain forms of clinical patterns of ENL evolve into one another form of aberrant presentation: for example, ENL can undergo central necrosis to evolve in ENL necroticans.
Atypical morphological presentations.8 of ENL like ENL necroticans(ulcerative), vesiculobullous, sweet syndrome like, erythema multiforme like, lucio phenomenon like,pustular lesions, vasculitis like and several other variants have already been described in literature.As ENL presents mimicking these conditions, it hampers the diagnostic process which accelerates the disease activity and possibly causes nerve damage. Consequently for that reason deep knowledge of these not so common aberrant presentations aids us in seamless diagnosis and management of type 2 lepra reaction.
We have noticed the trend of rise in several atypical variants and increase in severity of ENL in post covid era. COVID 19 infection.9 emerged as outbreak of pneumonia in wuhan, china and spreaded all over the world. The disturbing fact about the COVID pandemic is that possible effect of increase in the immunological events in the presence of infection as the trigger and the treatments implemented that interfere with inflammatory response of these patients.
Suspected cytokine storm and neutrophilia are hypothesized to be the cause in both these conditions. Therefore we aim to study the aberrant presentations of ENL and correlating it with possible triggers like COVID infection, vaccination, poor access to care and several others.
Materials and Methods
Ethical committee clearance was obtained. It is the retrospective observational case series study. Records of Erythema nodosum leprosum patients admitted as inpatient department of Government Stanley medical college, Chennai from January 2020 to December 2022 were collected and patients with aberrant presentations were analysed in terms of age, sex, onset of ENL episode, number of ENL episodes, spectrum of leprosy, morphology of lesions, systemic complications, bacteriological index, COVID status and treatment given.
History, examination and histopathology were used for diagnosis of erythema nodosum leprosum.
Chronic ENL was defined as the persistence of ENL for >6 months despite adequate treatment.
Recurrent ENL was defined as the occurrence of greater than 4 episodes in a year.
Severity of ENL was assessed by ENLIST scoring system.
ENL was diagnosed on the basis of Naafs criteria for type 2 reaction:
Table 0
Exclusion criteria
ENL patients not fulfilling Naafs criteria.
Patients with vascular disease, tuberculosis and connective tissue disorder.







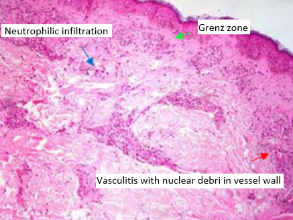
Table 1
Age distribution of study sample
|
Age in years |
Number of patients |
|
11- 20 |
0 |
|
21-30 |
2 |
|
30-40 |
9 |
|
40-50 |
4 |
|
51-60 |
3 |
|
>60 |
1 |
Table 2
Patient distribution on the basis of onset of type 2 reaction episode
|
Onset |
Number of patients |
|
After MBMDT |
|
|
Within 1 year |
7 |
|
1-2 year |
0 |
|
After 2 years |
0 |
|
During MBMDT(months) |
12 |
|
First 6 months |
9 |
|
Next 6 months |
3 |
Table 3
Clinical profile of sample population
Results
A total of 41 patients were admitted in the inpatient of Dermatology department of the tertiary hospital with ENL during the study period of 3 years. Out of these 19 patients (46.3%) had aberrant presentations of ENL.
Out of these 19 patients, 12/19(63%) were male and 7/19 (37%) were female..Age ranged from 30 to 40 years is the most common age group i.e., 9/19 (47%) [Table 2].
All patients were in the borderline lepromatous and lepromatous pole of the spectrum. 10/19 (52%) were in lepromatous spectrum and 9/19(48%) were in borderline lepromatous spectrum. High bacteriological index were noted 13/19 (68%) who had BI of > 4+.
Regarding the onset of ENL 12/19(63%) patients developed ENL during the course of MBMDT with particularly more number ENL onset during first 6 months of MBMDT therapy [Table 3].
4/19(21%) patients had ENL necroticans which is the commonest presentation in the study followed by ecthyma like ENL which is 2/19(10%) and sweet syndrome like ENL 2/19(10%).
7/19(36%) patients had recurrent ENL, 2/19(10%) had chronic ENL. Almost all patients 14/19(73%) has given the history of COVID infection prior to the onset of ENL and has underwent treatment. The mean ENLIST score of COVID infected individuals was 8 compared to mean ENLIST Score of covid non infected individuals which was 5.
4/19(21%) patients had history of COVID VACCINATION.
Histopathological examination revealed superficial and deep perivascular infiltrate of lymphohistiocytes, neutrophilic and foamy macrophages. Evidence of vasculitis and fibrin deposition were noted in all patients.
Sweet syndrome like ENL patient had HPE feature of edema of papillary dermis followed by neutrophilic infiltrate and vasculitis like features
Almost all patients had moderate to severe neuritis with the involvement of more than 1 nerve.7/19(36%) patients had grade 1 deformity. and 5/19(26%) patients had grade 2 deformity.
Systemic symptoms like fever and malaise were present in almost all the patients. 6/19(31%) patients arthritis and 4/19(21%) patients has tibial tenderness.
2/19(10%) patients had generalized edema, 1 /19(5%) had glomeronephritis and 1/19(5%) patient had iritis.
All the patients were started on oral prednisolone according to WHO guidelines.Thalidomide was used in 2/19(10%)chronic ENL patients.Azathioprine was used in 6/19(31%) patients.
MBMDT was initiated and restarted whenever required. ENL episode was controlled in all patients within 2 to 3 weeks after the treatment was initiated.
Clinical profile of patients in the study is enclosed [Table 4].
Discussion
Erythema nodosum leprosum. 10 also known as type 2 reaction is an immune complex mediated (type 3 hypersensitivity reaction ) reactional state encountered among borderline lepromatous and lepromatous leprosy either before during or after the institution of anti leprosy treatment. ENL is characterized by the eruption of tender evanescent subcutaneous nodules and constitutional symptoms like fever, malaise, arthralgia and myalgia.
Permanent nerve damage and deformities are the consequences of ENL. 11 Recently ENL is certainly on the rise due to increase in the number of multibacillary cases. Eventhough leprosy has been eliminated in 2005 there is more number of multibacillary cases reporting with ENL indicating the need for adequate awareness among both medical fraternity and community workers regarding the various presentations and importance of early diagnosis.
ENL has some known triggers. 12 such as lepromatous leprosy with bacillary index of >4+,antileprosy treatment,physical and mental stress,surgical intervention,pregnancy, parturition and intercurrent infections. There has been constant flow of newer insights in the pathogenesis of erythema nodosum leprosum. One such theory is the cytokine storm which is present in ENL. There is substantial evidence of rise in TNF alpha and IFN gamma in patients with ENL. IL -1,IL- 4,IL-6,IL-8,IL-10,IL-12 have also been involved. 13
As we discussed earlier, intercurrent infections can be trigger for ENL, the recent COVID pandemic. 14 may caused the rise in number of ENL cases. Studies shows that blood workup of COVID 19 patients showed wise WBC, neutrophil percentage, absolute neutrophil count and neutrophilic lymphocytic ratio. ENL is also considered as the neutrophilic immune complex mediated disease, there must be association with COVID being the trigger.
In our study we have noticed 14/19 patients has given history of COVID 19 infection prior to the onset of exacerbation.The mean ENLIST score of COVID affected individuals is significantly raised (ENLIST score- 8) compared to the COVID unaffected individuals (ENLIST score- 5) which showcases the effect of cytokine storm in erythema nodosum leprosum.
Study done by Zuo and colleagues. 15 demonstrated COVID 19 patients presented with rise in serum free DNA, MPO –DNA, CIT H3( citrullinated histone 3). The last two are markers of neutrophilic extracellular traps (NET). This further confirms interrelationship of neutrophils in the pathogenesis of ENL and COVID 19.
ENL necroticans is the commonest unusual presentation of ENL which constitutes 4/19 cases in our study. ENL necroticans is characterized by multiple tender nodules which undergo spontaneous ulveration with severe systemic symptoms. Verma and pandhi et al. 16 first reported the case of ENL necroticans.Lucio phenomenon must ne differentiated from ENL necroticans by absence of constitutional and systemic symptoms. In our patients it healed wit atrophic scars. On histopathalogical examination,we observed focal loss of epidermis in few areas,proliferation of vessels in dermis, diffuse neutrophilic infiltration around vessels. In hasija et al,17 they have reported a case which has overlapping features of both lucio phenomenon and ENL necroticans.
We have observed ecthyma like ENL in 2/19 cases. These patients had minimal systemic symptoms which includes arthralgia and intermittent fever. Both the patiemts had two to three lesions distributed over trunk and limbs. They were on corticosteroids for treatment of recurrent ENL. As they were immunosupressed bacterial infection was suspected and they were treated with antibiotics. Due to non regression of the lesion,biopsy was done which exhibits diffuse neutrophilic infiltration and vasculitis.
Sweet syndrome like ENL was noticed in 2/19 cases on our study. it is characterized by sudden appearance of evanescent crops of erythematous tender nodules and plaques. These plaques may contain pseudovesicles due to severe edema of papillary dermis. Kuo and chan. 18first reported the case of sweet syndrome like ENL.
Histopathology of ENL shows edema of papillary dermis,superimposed infiltration of fragmented and intact neutrophils. only one case revealed features of vasculitis. According to Chavez alvarez et al. 19,which is the systematic review of literature of available online case series and reports, sweet syndrome like ENL is the most common atypical presentation of ENL which constitutes 21 cases.
Type 1 reaction and type 2 reaction coexisted in one patient with borderline lepromatous hansen.he was a case of recurrent ENL on azathioprine,he developed raised erythematous plaque along with systemic symptoms.on histopathology, foam cells and histiocytic collection with ill defined granuloma formation and neutrophilic infiltration. According to debajyoti et al. 20, in which they have done biopsy for 20 doubtful cases with overlapping features of type 1 and type 2 reaction, majority of the cases had histological features of ENL.
Erythema multiforme like lesions was noted on one case of borderline lepromatous leprosy treated and rel eased from treatment 5 months back. It started as erythematous plaques with after few days gives central hyperpigmenation giving targetoid appearance.Absence of palmoplantar lesions and mucosal lesions helps in differentiating from classic EMF. On histopathological examination pandermal perivascular, periadnexal and periappendageal lymphohistiocytic infiltrates with foamy histiocytes were noted. In kabir sardana et al. 21, a case of late leprosy reaction presenting as EMF like ENL with underlying rifampicin resistance and its potential implications have been described.
Fixed drug eruption like ENL was noted in one patient in our study. Patient presented with hyperpigmented lesion with erythematous hue, due to absence of drug history and persistence of erythema along with systemic symptoms for few weeks, biopsy was done on hpe,we observed diffuse neutrophilic infiltration. on treatment with systemic corticosteroids, systemic symptoms resolved followed by healing of the leasion with hyperpigmentation.
Psoriasiform ENL was noted in one case of ENL. Patient features of lepromatous leprosy and was on MBMDT.He developed multiple well defined erythematous tender psoriasiform plaques along with systemic symptoms which on histopatholical examination revealed diffuse infiltration of neutrophils in the dermis along with foamy macrophages. In Bhagyashree supekar et al.. 22 they have reported a case of of atypical psoriasiform presentation of LL but not with reaction. In our study we are reporting a case of psoriasiform variant of ENL which is never described in literature so far to our knowledge.
Vesiculobullous ENL was noted in one case of ENL.histopathological examination revealed subepidermal bulla with diffuse neutrophilic infiltrates.
Sethuraman et al. 23 reported a case of ENL with bullous lesions.sparing of oral mucosa,presence of classical ENL lesions along with bullous lesions, absence of acantholytic cells in tzanck and immunoflurorescence helps in diagnosis.
One patient presented with lymphadenopathy in b/l cervical and axillary lymph nodes with systemic symptoms like fever and arthralgia.He was previously treated as a case of TB lymphadenopathy with ATT and was referred because he has recurrent lympahadenopathy and systemic symptoms. On examination, diffuse skin infiltration and madarosis was noted.on SSS BI of 5+ was obtained. In goyal et al. 24, they have reported a case of lymph node abcess and cardiac involvement in a case of LL Hansen with ENL.
In Wankhede et al. 25, a retrospective study of uncommon variants of erythema nodosum leprosum the most common presentation is ENL necroticans similar to our study.
Aberrant presentations of ENL causes delay in the diagnosis because most of the cases were treated by primary care physicians during the COVID period. They were symptomatically treated for fever, joint pain and periodically tested by COVID PCR for few weeks. Some cases with vesiculobullous,sweet syndrome like and EMF like lesions were considered separate entity and they got treated at peripheral hospitals. The period of the delay varies depended on the duration between referral to tertiary care.
Conclusion
Erythema nodosum leprosum can present in various atypical forms.Aberrant presentations of erythema nodosum leprosum always pose a problem in appropriate timely diagnosis and management.This study emphasizes the need for healthcare professionals to be aware of varied atypical presentations of erythema nodosum leprosum especially leprosy endemic countries. This study also correlates the atypical presentation of erythema nodosum leprosum attributable to C0VID 19 infection which might act as trigger and contribute to cytokine storm.
Abbreviations
ENL – Erythema Nodosum Leprosum; EMF – Erythema Multiforme; COVID – Corona Virus Disease; ENLIST Severity scale – ENL International Study Group Severity scale; MBMDT – Multi Bacillary Multi Drug Therapy; WHO – World Health Organisation; LL – Lepromatous Leprosy; TB –Tuberculosis; ATT- Anti Tuberculous Treatment; SSS – Slit Skin Smear.