- Visibility 395 Views
- Downloads 40 Downloads
- Permissions
- DOI 10.18231/j.ijced.2025.017
-
CrossMark

Clinico-demographical profile and correlation of cardiff acne disability index score (CADI) and Global acne grading system score (GAGS) in patients with acne vulgaris in a tertiary health care centre
- Author Details:
-
 Vaddadi Akhila Vara Madhuri *
Vaddadi Akhila Vara Madhuri *
-
Neena Reddy
-
Gopalakrishnan Kunjaram
-
Jayakar Thomas
Abstract
Background: Acne is a chronic, self-limiting inflammatory disease of pilosebaceous unit. It is multifactorial, affects at least 85% of teenagers and young adults with dermatological and psychological effect too. The current study focuses on clinico-demographic characteristics of patients with acne vulgaris and correlation of Cardiff acne disability index score (CADI) and Global acne grading system score (GAGS) in patients attending the outpatient department of dermatology at a tertiary care hospital, in southern India.
Materials and Methods: A Cross sectional study conducted in 170 adult patients diagnosed with acne vulgaris attending OPD of Dermatology in a teaching hospital. Institutional ethical clearance and patient’s consent was taken. Pregnant and lactating women, patients who are hypersensitive to retinoids and presented with any other skin condition that would interfere with diagnosis or assessment of acne were excluded from the study. Data on clinico-demographic characteristics, Cardiff acne disability index (CADI) score and Global acne grading system- GAGS of patients was obtained using a semistructured questionnaire. Statistical analysis done using, chi-square, t test and pearsons correlation with P<0.05 considered as statistically significant in SPSS version 22.
Results: Majority of the participants were females (71.8%), and between the age group 26 to 32 years (36.5%) followed by 18 to 25 years (27.6%), with 61.2% found to be unmarried. The cheeks (95.3%) were the most common site of involvement, followed by forehead (51.2%). Chi-square shows significant association with younger age and females (P<0.05). CADI score is positively correlated with GAGS score (pearsons rho = 0.81 with P<0.05).
Conclusion: Gender and age are significant demographic factors associated with acne, CADI score is positively correlated with GAGS score, thus showing effect of acne on quality of life.
Introduction
Acne is one of the most common skin diseases seen in clinical practice and is caused by multiple factors which originates in the pilosebaceous follicle.[1], [2] Acne is characterized by seborrhoea, the formation of open and closed comedones, erythematous papules, and pustules and in more severe cases nodules, deep pustules and pseudocysts.[3] It is a multifactorial disease depending on genetic predisposition, endocrine factors, follicular epidermal hyperproliferation, excess sebum production, inflammation, the colonization and activity of Propionibacterium acnes, and environmental factors. Several agents were used in management due to its multifactorial pathogenesis to offer higher benefit to patients. [4]
Scientific advances are continually improving the knowledge of acne and contributing to the refinement of treatment options; it is important for clinicians to regularly update their practice patterns to reflect current standards.[5] Several scoring systems are available to grade the severity of acne, of which Global acne grading system score (GAGS) is easy to administer.
Acne vulgaris remains as a chronic condition affecting the self-esteem of the patients. It has been found to have a significant negative impact on the health-related QoL as stated by several previous studies.[6], [7] Acne vulgaris's impact on quality of life can be measured using the Cardiff Acne Disability Index (CADI). Though impairment in the quality of life of patients of acne vulgaris is well established, its direct correlation with clinical severity has not been established. Hence the current study was undertaken to understand the clinicodemographic profile and effect of severity of acne vulgaris on psychological status of the patient.
Objectives
To assess clinic-demographical profile of patients with acne vulgaris.
To correlate the effect of severity of acne (by GAGS index) on quality of life (by CADI score).
Materials and Methods
A Cross sectional study was done in patients with clinically diagnosed acne vulgaris, attending the outpatient department of teaching hospital from January 2023 to November 2023.
Inclusion criteria
Adult patients of either sex with clinical diagnosis of acne vulgaris. Patients who are willing to participate in the study, to undergo required laboratory investigations were included in the study.
Exclusion criteria
Pregnant and lactating women, patients who are hypersensitive to retinoids and presented with any other skin condition that would interfere with diagnosis or assessment of acne were excluded from the study.
Patients were selected by purposive sampling method.
Sample size was calculated using formula for finite population. Where, Z α is the standard normal deviate, 1.96 at 95% confidence interval.
As per previous medical records from our department acne vulgaris form almost 20% of all cases attending dermatology OPD.
Hence P = Prevalence is 20%. i.e P = 0.2, 1-P = (1-0.2)
e = allowable error was 5% (i.e 5% of prevalence was considered)
N = study population (Patients with acne vulgaris who attended dermatology OPD in the institution in the previous year) = 200,
Sample size(n)= z2X p(1-p)e21+z2X p(1-p)e2N Sample size(n)= (1.96)2X 0.2(1-0.2)(0.05)21+(1.96)2X 0.2(1-0.2)(0.05)2 200 Sample sizenrequired is=130After obtaining institutional ethical committee clearance and informed consent from patients. Data was collected on clinico demographic details. Clinical examination and Routine investigations were done. Acne vulgaris was graded using Global acne grading system score (GAGS).[8] An online simple Global acne grading system score (GAGS) calculator was used. This system divides the face, chest and back into six areas (forehead, each cheek, nose, chin and chest and back) and assigns a factor to each area on the basis of size. It has a score range of 1-44, with mild acne being 1-18, moderate acne being 19-30 and severe acne being 31-44. ([Table 1])
|
Location |
Factor |
|
Forehead |
2 |
|
Right cheek |
2 |
|
Left cheek |
2 |
|
Nose |
1 |
|
Chin |
1 |
|
Chest and upper back |
3 |
English version of the Cardiff Acne Disability Index (CADI) 2021 updated version– a well validated acne instrument derived was used for assessment of quality of life. [9] The Cardiff Acne Disability Index (CADI) is a simple questionnaire for assessing the disability caused by acne. It consists of 5 questions dealing with interference in life functions or psychosocial adjustment caused by acne, which are graded from 3 (greatly) to 0 (none) with higher scores indicating greater impairment. The score ranges from 0-15 with mild impact, moderate impact and severe impact being 0-4, 5-9, and 10-15 respectively (shown in table 2). Data was entered in semi structured questionnaire.
|
As a result of having acne, during the last month have you been aggressive, frustrated or embarrassed? |
• Very much indeed |
|
|
• Very much indeed |
|
|
• A lot |
|
|
• A little |
|
|
• Not at all |
|
Do you think that having acne during the last month interfered with your daily social life, social events or intimate personal relationships? |
• Severely, affecting all activities |
|
|
• Moderately, in most activities |
|
|
• Occasionally or in only some activities |
|
|
• Not at all |
|
During the last month have you avoided public changing facilities or wearing swimming costumes because of your acne? |
• All of the time |
|
|
• Most of the time |
|
|
• Occasionally |
|
|
• Not at all |
|
How would you describe your feelings about the appearance of your skin over the last month? |
• Very depressed and miserable |
|
|
• Usually concerned |
|
|
• Occasionally concerned |
|
|
• Not bothered |
|
Please indicate how bad you think your acne is now: |
• The worst it could possibly be |
|
|
• A major problem |
|
|
• A minor problem |
|
|
• Not a problem |
Statistical analysis: Data entered in Microsoft excel 2019 and represented in tables and graphs. Quantitative variables were described using percentages, ranges, means and standard deviations. SPSS version 22 was the statistical software used. Students t test, chisquare test, Anova test and pearsons correlation was used for statistical analysis with P<0.05 as statistically significant.
Results
|
Patients’ characteristics |
Frequency (n=170) |
Percent (%) |
|
|
Age Group |
18 to 25 |
47 |
27.6% |
|
26 to 32 |
62 |
36.5% |
|
|
33 to 39 |
34 |
20.0% |
|
|
40 to 45 |
27 |
15.9% |
|
|
Sex |
Male |
48 |
28.2% |
|
Female |
122 |
71.8% |
|
|
Marital status |
Married |
66 |
38.8% |
|
Unmarried |
104 |
61.2% |
|
|
Occupation |
Housewives |
65 |
38.2% |
|
Students |
47 |
27.6% |
|
|
Self employed |
58 |
34.1% |
|
|
Comorbidities |
Diabetes Mellitus type 2 |
12 |
7% |
|
Thyroid disorders |
15 |
8.8% |
|
|
Hypertension |
4 |
2.3% |
|
|
Hyperlipidaemia |
9 |
5.3% |
|
|
Anaemia |
25 |
14.7% |
Majority of the participants were females (71.8%), and between the age group of 26 to 32 years (36.5%) followed by 18 to 25 years (27.6%), with 61.2% found to be unmarried. Housewives were 38.2% and others were self-employed 34.1% and students were 27.6%. Comorbidities included DM type 2, thyroid disorders, hypertension, hyperlipidaemia and anaemia in 7%, 8.8%, 2.3%, 5.3% and 14.7% respectively. ([Table 3])
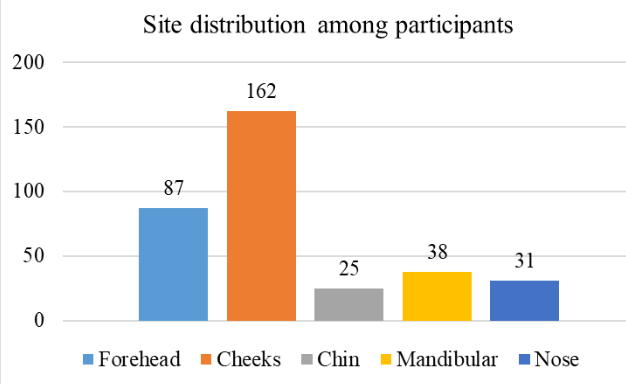
The cheeks were found to be the most common site of involvement in cases of acne, with 95.3% of cases which showed lesions followed by forehead (51.2%). ([Figure 1])
|
GAGS and CADI score |
Mean ± SD/ Range |
Sub group |
Frequency |
Percentage |
|
Global acne grading system score (GAGS) |
34.8 ± 15.8/ 4-39 |
Mild acne (0-18) |
25 |
14.7 |
|
Moderate acne (19-30) |
48 |
28.2 |
||
|
Severe acne (31-44) |
97 |
57.1 |
||
|
Cardiff acne disability index score (CADI) |
8.7 ± 3.4/ 1-13 |
Mild impact (0-4) |
34 |
20 |
|
Moderate impact (5-9) |
47 |
27.6 |
||
|
Severe impact (10-15) |
89 |
52.4 |
Mean and SD of GAGS and CADI scores of the study population was 34.8 ± 15.8 and 8.7 ± 3.4. As per GAGS majority of patients had severe acne (97/57.1%) followed by moderate (48/28.2%) and mild acne (25/14.7%). The impact on quality of life as per CADI in the study population was mild in 34(20%) patients, moderate in 47(27.6%) patients and severe in 89(52.4%) patients. ([Table 4])
|
GAGS score (n) |
Mean (SD) CADI |
Range |
Anova test/ p value |
Pearsons’s correlation coefficient / P value |
|
Mild acne (25) |
4.3(1.1) |
1-5 |
321/ <0.05 |
0.81/<0.05 |
|
Moderate acne (48) |
7.1(1.3) |
5-9 |
||
|
Severe acne (97) |
10.2(1.5) |
9-13 |
||
|
Total |
8.7(3.5) |
1-13 |
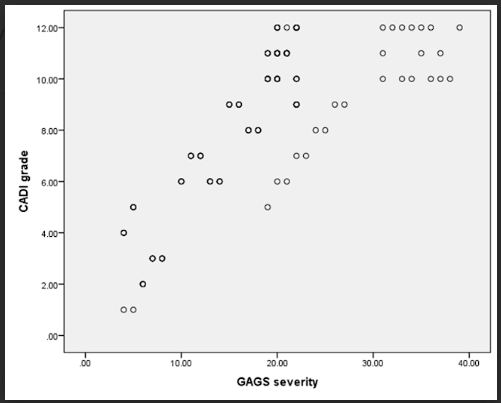
The overall mean and Sd in this study was 8.7 and 3.5, with a range of 1-13. The mean of CADI was 4.3, 7.1and 10.2 in patients belonging to group of mild acne, moderate acne and severe acne and this difference was significant statistically (P<0.05). Pearsons’s correlation coefficient shows very strong positive correlation between GAGS and CADI (rho-0.81/ p <0.05). ([Table 5] and [Figure 2]).
|
Characteristics |
Mild acne (25) |
Moderate acne (48) |
Severe acne (97) |
Chi-square or t test/ P value |
|
|
Age in years (mean ± SD) |
39.7±11.9 |
32.3±8.9 |
24.2±12.8 |
2.19/0.03 |
|
|
Gender |
Male (48) |
12 (25%) |
19(39.6%) |
17(35.4%) |
13.3/0.0012 |
|
Female (122) |
13 (10.7%) |
29(23.8%) |
80 (65.5%) |
||
|
Marital status |
Married (66) |
8 (12.1%) |
21(31.8%) |
37(56.1%) |
0.9/0.6 |
|
Unmarried (104) |
17(16.3%) |
27(56.2%) |
60(61.5%) |
||
|
Duration of acne in years (mean ± SD) |
5.7±2.9 |
7.2±5.9 |
6.1±3.4 |
1.36/0.17 |
|
|
Haemoglobin in g/dl(mean ± SD) |
11.3±2.9 |
10.9±1.6 |
11.4±2.3 |
0.58/0.91 |
|
|
HbA1c (%) |
5.5±1.2 |
5.9±2.7 |
6.3±3.5 |
0.78/0.41 |
|
|
Free T3 (pg/ml) (mean ± SD) |
3.11±2.1 |
3.2±1.3 |
2.9±1.5 |
0.71/0.473 |
|
|
Free T4 (μg/dl) (mean ± SD) |
5.6±2.7 |
5.9±1.9 |
6.7±1.1 |
1.3/0.2 |
|
|
Total cholesterol (mg/dl) (mean ± SD) |
156±19.8 |
172±13.5 |
163±21.7 |
1.37/0.10 |
|
|
HDL cholesterol (mg/dl) (mean ± SD) |
37±16.7 |
34±11.7 |
35±19.1 |
0.79/0.42 |
|
|
LDL cholesterol (mg/dl) (mean ± SD) |
106.2±14.7 |
94±14.2 |
109.9±15.4 |
1.7/0.08 |
Mean age of patients with mild, moderate and severe acne were 39.7, 32.2 and 24.2 years, this shows that mean age was less in patients with severe acne, which was significant statistically. More proportion of females (65.5%) compared to males (35.4%) had severe acne and this difference was significant statistically. Marital status, mean of duration of acne, mean haemoglobin, mean HbA1c levels, mean free T3 and free T4 and mean of HDL, LDL and total cholesterol showed no significant difference with severity of acne. Thus, only age and gender were significantly associated with severity of acne. ([Table 6])
Discussion
Acne vulgaris is chronic inflammatory condition of thr pilo-sebaceous unit with a prolonged course, a pattern of recurrence or relapse, manifesting as acute outbreaks or slow onset, and a psychological and social impact on the individual's quality of life. Emotional effects such as embarrassment, decreased self-esteem, and difficulties in relationship building were observed in a considerable percentage of acne-affected individuals. Thus, importance of early identification and treatment to mitigate the long-term socio-economic impact of acne is needed. The assessment on the intricate interplay between acne vulgaris, psychological factors, and quality of life, guides dermatologists, advocating for a comprehensive treatment strategy that not only targets the clinical aspects of the condition to enhance the general well-being of the affected individuals.
In this study majority of the participants were females (71.8%), and between the age group of 26 to 32 years (36.5%) followed by 18 to 25 years (27.6%), with 61.2% found to be unmarried. In study by Budamakuntla L et al, the most common age group involved was 18-25 years (55.7%) while it was 16-20 years (59.8%) in the study by Thappa et al.[10], [11] In study by Singh A et al there was 40% males and 60% females, and mean age of the study population was 20.33±4.05 years with maximum number of patients belonged to the age group 16-20 years (63%). [12] In study by Raghavan J S et al, out of the 100 patients 74% were women and 26% were men. The age of patients varied from 11-45 years with a mean age of 23.09 years. The most common age group involved was 21-25years (38%), followed by16-20 years (32%). [13] In study by George RM mean age of patients was around 30.9±5.4. The youngest patient was 26-year-old and the oldest one was 49 years. Sixty-nine (62.7%) patients in this study were in the age group between 26 and 30 years followed by 18 patients (16.4%) in the age group 31–35 years. Forty-six patients (41.8%) had a duration of <5 years whereas 14 (12.7%) patients had a total duration of >15 years. Out of the 110 patients included in the study by George et al, 89 (80.9%) were female and 21 (19.1%) were male.[14] This differences across studies were due to enrolment of different age groups and study setting. In various age groups, women experience acne more frequently than men do, and it seems to begin earlier in women, which could be connected to their earlier puberty. However, in their late teens, men experience more severe acne than females, which is consistent with androgens being a powerful stimulator of sebum production in this age range. While female acne usually appears as a less severe yet persistent kind, male acne usually appears later in puberty and is more severe.
In this study the cheeks were found to be the most common site of involvement in cases of acne, with 95.3% of cases showing lesions followed by forehead (51.2%). In the Study by Singh A et al all the subjects (100%) had lesions on face, 23 (7.7%) had lesions on face and back and 7 patients (2.3%) had lesions on face, back and chest. [12] In study by Raghavan et al, face was affected in all patients with cheeks in 91%, forehead in 72%, mandible in 36% and chin in 28% patients. Trukal involvement was less with chest in 10%, back in 13%, shoulder in 8% and upper arm in 3%.[13] Our study findings were comparable to other studies with commonest site involved as face, which has the highest density of sebaceous follicles.
As per GAGS majority of patients had severe acne (97/57.1%) followed by moderate (48/28.2%) and mild acne (25/14.7%) in this study. In study by Gupta A et al, the overall mean global acne grading system score was 21.43 (±6.73, range 10–40). Mild, moderate, severe and very severe acne were present in 44%, 42%, 12% and 2% of the patients, respectively.[15] In the Study by Singh A et al 15 (20.0%) patients had grade 1 acne, 25 (33.3%) had grade 2, 20 (26.7%) had grade 3 and 15 (20.0%) had grade 4 acne. (12) As per study by Lakshminarayana K et al maximum patients presented with Grade II acne (61 %) followed by grade III (27%). Grade IV (severe) seen in few cases. [16] All the studies have similar findings showing that majority had severe acne as the likelihood of seeing dermatologists was found to be connected with the severity of acne, moreover patients with mild acne probably preferred over the counter medications or home remedies.
The impact on quality of life as per CADI in the study population was mild in 34(20%) patients, moderate in 47(27.6%) patients and severe in 89(52.4%) patients in the current study. The overall mean and SD in this study was 8.7 and 3.5, with a range of 1-13. In this study the mean of CADI was 4.3, 7.1and 10.2 in patients belonging to group of mild acne, moderate acne and severe acne and this difference was significant statistically. In study by Gupta et al, the overall mean Cardiff acne disability index was 6.09 (±3.153, range 0–15).[15] The CADI score in our study was higher, probably because it was conducted at a referral institution.
Quality of life based on CADI shows very strong positive correlation with GAGS [Pearsons’s correlation coefficient between GAGS and CADI (rho-0.81/ <0.05)]. Impact on QOL is severe with increasing severity of acne vulgaris in our study. Our finding was similar to finding with study by Gupta et al which shows, Pearsons’s correlation coefficient between GAGS and CADI (r = 0.83). [15] As per study by Lakshminarayana K et al according to the scoring - 1% had no effect on their life, 15% had a small effect on their life, 16% had a moderate effect on their life, 59% of patients had a large effect on their life (p 0.000), 9% had an extremely large effect on patients’ life which was similar to current study. [16]
In this study mean age of patients with mild, moderate and severe acne were 39.7, 32.2 and 24.2 years, this shows that mean age was less in patients with severe acne, which was significant statistically. More proportion of females (65.5%) compared to males (35.4%) have severe acne and this difference was significant statistically. In contrast study by Singh A et al showed that there was no significant difference in the grade of acne between males and females though grade 2 was more common among males and grade 1 was more common among females. These differences could be attributed to the type of patients presenting to each centre. Females have earlier onset of acne as compared to males. [11] Severe grades of acne were more in females, 46% compared to16% in males, and this is almost similar to the results of previous studies and our study. [8], [17], [18]
Conclusions
Quality of life based on CADI shows very strong positive correlation with GAGS. Impact on QOL is severe with increasing severity of acne vulgaris. The study emphasises the need for dermatologists to consider the QoL aspects of individuals with acne and suggests that interventions should be tailored to individual traits and impairments. This could be by, in-depth counselling and psychotherapy as well as psycho-pharmacotherapy when and where required by a psychiatrist. Dermatologists should be mindful of psychological morbidity, stressing the significance of integrated psychosomatic treatment in acne management. Future research should consider confounding factors and broaden demographic representation for a more comprehensive understanding.
Source of Funding
None.
Conflict of Interest
None.
References
- Williams H, Dellavalle R, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-72. [Google Scholar]
- Bhat S, Deshmukh G, Dhoot D, Barkate H. Comprehensive Skin Care Regimen of Moisturizer with BroadSpectrum Sunscreen as an Adjuvant in Management of Acne (CHARISMA). Int J Sci Stud. 2018;6(5):5-9. [Google Scholar]
- Layton A, TB, SB, Cox N, CG. Disorders of the sebaceous glands. Rook's Textbook of Dermatology. 2010. [Google Scholar]
- Kosmadaki M, Katsambas A. Topical treatments for acne. Clin Dermatol. 2017;35(2):173-8. [Google Scholar]
- Thiboutot D, Dréno B, Abanmi A, Alexis A, Araviiskaia E, MC. Practical management of acne for clinicians: An international consensus from the global alliance to improve outcomes in acne. J Am Acad Dermatol. 2018;78(2 Suppl 1):1-23. [Google Scholar]
- Golics C, Basra M, Finlay A, Salek M. Adolescents with skin disease have specific quality of life issues. Dermatology. 2009;218(4):357-66. [Google Scholar]
- Ogedegbe E, Henshaw E. Severity and impact of acne vulgaris on the quality of life of adolescents in Nigeria. Clin Cosmet Investig Dermatol. 2014;7:329-34. [Google Scholar] [Crossref]
- Adityan B, Kumari R, Thappa D. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol. 2009;75(3):323-6. [Google Scholar]
- Motley R, Finlay A. Practical use of a disability index in the routine management of acne. Clin Exp Dermatol. 1992;17(1):1-3. [Google Scholar]
- Budamakuntla L, Parasramani S, Dhoot D, Deshmukh G, Barkate H. Acne in Indian population: An epidemiological study evaluating multiple factors. IP Indian J Clin Exp. 2020;6(3):237-42. [Google Scholar]
- Thappa DM, Balaji A. Profile of acne vulgaris-A hospital-based study from South India. Indian J Dermatol Venereol Leprol. 2009;75(3):272-8. [Google Scholar]
- Singh A, Dhillion K. ClinicoEpidemiological Profile of Acne in Northern India. Ann Int Med Den Res. 2019;5(3):6-8. [Google Scholar]
- Raghavan J, Fathima S, Ameera S, Muhammed K. Clinical profile of acne vulgaris: an observational study from a tertiary care institution in Northern Kerala, India. Int J Res Dermatol. 2019;5(3):476-80. [Google Scholar]
- George R, Sridharan R. Factors aggravating or precipitating acne in Indian adults: A hospital-based study of 110 cases. Indian J Dermatol. 2018;63(4):328-31. [Google Scholar]
- Gupta A, Sharma Y, Dash K, Chaudhari N, Jethani S. Quality of life in acne vulgaris: Relationship to clinical severity and demographic data. Indian J Dermatol Venereol Leprol. 2016;82(3):292-7. [Google Scholar]
- Lakshminarayana K. Clinico-Epidemiological Study of Acne Vulgaris and Quality of Life Assessment. Sch J App Med Sci. 2018;6(7):2863-8. [Google Scholar]
- Kane A, Niang S, Diagne A, Ly F. Epidemiologic, clinical, and therapeutic features of acne in Dakar, Senegal. Int J Dermatol. 2007;46(1):36-8. [Google Scholar]
- Adityan B, Thappa D. Profile of acne vulgaris--a hospital-based study from South India. Indian J Dermatol Venereol Leprol. 2009;75(3):272-8. [Google Scholar]