- Visibility 582 Views
- Downloads 55 Downloads
- Permissions
- DOI 10.18231/j.ijced.2022.035
-
CrossMark

The study of epidemiological, clinical, histopathological and dermoscopic features of chronic plaque psoriasis
- Author Details:
-
 Laxmi Horatti
Laxmi Horatti
-
Dilip N R Kumar *
-
Shashikiran AR
Abstract
Background: Psoriaisis is a common papulosquamous condition seen by the dermatologists. It can involve the skin and nails. There are many sub types of Psoriasis with various clinical, histopathological and dermoscopic features. In this study we intend to study the epidemiological, clinical, histopathological and dermoscopic features of Chronic Plaque Psoriasis (CPP).
Materials and Methods: A total of 45 patients of CPP, above the age of 18 years who qualified the inclusion and exclusion criteria were included in the study. A proforma of epidemiological details was noted, clinical and dermoscopic examination of the lesions were done. The punch biopsy specimens of cutaneous lesions were subjected to histopathological examination and the findings noted.
Results: Out of the 45 patients included in the study, 31 were males and 14 females with a ratio of 2.21:1. The commonest symptom at presentation was flaking of skin and the most common site of involvement was trunk. On dermoscopic examination, dotted vessels and white scales were seen in all the patients. Hyperkeratosis, Parakeratosis, Acanthosis, Munro’s microabscess, Hypogranulosis were the significant histopathological features.
Conclusion: Psoriasis is more common in young adults and shows a male preponderance. Presence of dotted vessels in a regular distribution on dermoscopy is classical of CPP. Hyperkeratosis, Hypogranulosis and Munro’s microabscess are notable features of histopathology of LP.
Introduction
Psoriasis is a chronic, inflammatory and proliferative skin condition characterized by raised, well-defined, erythematous skin lesions surmounted by silvery-white scales. The disease is variable in duration, severity and morphology. Chronic plaque psoriasis (CPP) is the most common presentation of psoriasis. It presents as small to large, well-demarcated, red, scaly plaques.[1] Prevalence rate of psoriasis varies from 0% to 11.8% among different populations, in India it varies from 0.44 to 2.8%.[2] The most important diagnostic features of psoriasis are spongiform pustule and Munro microabscess.[3]
Dermoscopy is a non-invasive diagnostic modality which enables the visualization of morphologic features of skin that are otherwise invisible to the naked eye, thus forming a bridge between macroscopic clinical dermatology and microscopic dermatopathology. Dermoscopic patterns of many inflammatory skin diseases have already been described and it has been considered to be of high diagnostic accuracy for differentiating between common inflammatory skin disorders such as psoriasis and Lichen Planus.[4]
Homogenously distributed dotted vessels throughout the lesion over a typical light red background along with diffuse white scales has a high predictivity of CPP.[4], [5], [6], [7], [8]
Our study intends to throw some light on the epidemiological, clinical, dermoscopic and histopathological features in patients of CPP.
Materials and Methods
This was a prospective, cross-sectional study conducted in our dermatology OPD over the period of 1 year (From December 2018 to November 2019). Sample size was calculated to be 45 using n=Za2pq/E2, considering 5% prevalence of CPP (Where Za= 1.96 at 95% confidence level, E=0.05). Informed consent was taken from all patients prior to inclusion into the study.
A total of 45 newly diagnosed Psoriasis patients were included in the study. The inclusion and exclusion criteria were as under:
Inclusion criteria
Patients who were willing to give informed written consent for enrolment into the study.
Patients diagnosed with Psoriasis.
Exclusion criteria
Patients of age < 18 years.
Patients diagnosed with malignancies or other immunocompromised states.
Pregnant patients.
Detailed history was elucidated and complete cutaneous, mucosal and hair examination was done in all the patients. Dermoscopy of all cutaneous lesions were done using Dermlite DL3 (Figure 1) and photographed using Canon Ixus camera. Baseline investigations such as complete blood count, liver function test, renal function tests and skin/mucosal biopsy of the affected lesions were done. The histopathological assessment and reporting were done by pathologists.
Results
A total of 45 patients were recruited, out of which 31 were males and 14 females with a ratio of 2.21:1. The patients in 18 to 30 years age group were the majority (48.9%), followed by 31 to 40 years (20%), 41 to 50 years (17.8%) and least (13.3%) was in the patients over 51 years of age. The mean age of patients included in the study was 34.44 years. In our study 17 patients had associated comorbidities including diabetes mellitus (DM) in 11 patients (7 patients also had co existing hypertension (HTN)), only HTN in 2 patients and bronchial asthma in 5 patients. During the study period, 4 patients (8.9%) were also found to have associated Psoriatic Arthritis.





|
Variable |
Number of Patients (n=45) |
Percentage (%) |
|
Age Group |
|
|
|
18-30 |
22 |
48.9 |
|
31-40 |
9 |
20 |
|
41-50 |
8 |
17.8 |
|
>50 |
6 |
13.3 |
|
Sex |
|
|
|
Male |
31 |
68.9 |
|
Female |
14 |
31.1 |
|
Duration of symptoms |
|
|
|
<3 months |
27 |
60 |
|
3-6 months |
9 |
20 |
|
6-12 months |
7 |
15.6 |
|
>12 months |
2 |
4.4 |
|
Treatment taken before |
|
|
|
Yes |
21 |
46.7 |
|
No |
24 |
53.3 |
|
Family history of psoriaisis |
|
|
|
Yes |
6 |
13.3 |
|
No |
39 |
86.7 |
|
Associated conditions |
|
|
|
Diabetes Mellitus |
11 |
24.4 |
|
Hypertension |
9 |
20 |
|
Psoriatic Arthritis |
4 |
8.9 |
|
Bronchial Asthma |
5 |
11.1 |
|
Variable |
Number of Patients (n=45) |
Percentage (%) |
|
Symptom |
|
|
|
Itching |
36 |
80 |
|
Flaking of skin |
43 |
95.6 |
|
Redness |
32 |
71.1 |
|
Pain |
6 |
13.3 |
|
Sites involved |
|
|
|
Upper Limbs |
25 |
55.6 |
|
Lower Limbs |
28 |
62.2 |
|
Scalp |
6 |
13.3 |
|
Trunk |
39 |
86.7 |
|
Nails |
5 |
11.1 |
The duration of symptoms of less than 3 months was the commonest which was seen in 27 patients (60%), followed by 3 to 6 months duration in 9 patients (20%), 6 to 12 months duration in 7 patients (15.6%) and more than 12 months duration was seen in 2 patients (4.4%). The mean duration of symptoms in the patients included in the study was 4.58 months. Six patients (13.3%) in our study had a family history of Psoriasis. Demographic features are listed in [Table 1].
The commonest symptom was flaking of skin which was seen in 43 patients (95.6%), followed by itching in 36 patients (80%). Most common site of involvement was trunk, seen in 39 (86.7%) patients. Nail involvement was seen in 5 patients (11.1%). Pitting, Oil spots, Leuconychia, Subungual Hyperkeratosis were seen in these patients. ([Table 2])
On dermoscopic examination, dotted vessels were seen in all 45 patients (100) and in addition, red globules were seen in 8 patients (17.8%), the most common arrangement was in a regular distribution, seen in 43 patients (95.6%) and were associated with white scales in all (100%) cases.
Histopathological examination of all the biopsy specimens showed Hyperkeratosis, Parakeratosis, Acanthosis, Munro’s microabscess, Hypogranulosis, dilated vessels and perivascular infiltrate.
Discussion
Our study intended to elucidate the clinical histopathological and dermoscopic features of CPP. Psoriasis is a chronic, inflammatory and proliferative skin condition in which, the genetic and environmental influences have an etiological role. It is characterized by raised, well-defined, erythematous skin lesions surmounted by silvery-white scales. [1]
It was recognized as an entity distinct from leprosy by Robert Willan in the early 19th century and named by Ferdinand Hebra in 1841. The impact of Psoriasis on quality of life is still far-reaching and profound in modern times, even in the absence of stigmatization. [9]
Prevalence rate of psoriasis varies from 0% to 11.8% among different populations, in India it varies from 0.44 to 2.8% but the exact prevalence is not known. [10] For calculation of sample size we considered the prevalence to be 3% since it was the highest ever shown in Indian studies.
Chronic plaque psoriasis, the most predominant variant, is characterized by well-defined erythematous papulosquamous lesions ([Figure 2], [Figure 3]). The entire body surface may occasionally be involved (erythrodermic psoriasis) or multiple, small, widely disseminated papules and plaques are seen (guttate psoriasis). Less often, multiple pustules may be seen in generalized pustular psoriasis and pustulosis of the palms and soles. [1], [2]
Removal of the superficial silvery white scales via curettage (Grattage method), reveals a typical coherence, similar to the scraping on a wax candle (‘signe de la tache de bougie’). On further scraping, a glistening membrane (Membrane of Bulkeley) is seen, which on removal, presents with a characteristic pinpoint bleeding (Auspitz sign). [1], [2]
Nail psoriasis may be associated with cutaneous psoriasis with features such as Pitting, Onycholysis, Oil spots, Leuconychia, Sunungual hyperkeratosis etc ([Figure 4]).[11]
In our study, patients in 18 to 30 years age group were the majority (48.9%), followed by 31 to 40 years (20%), 41 to 50 years (17.8%) and least (13.3%) was in the patients over 51 years of age. The duration of symptoms of less than 3 months was the commonest which was seen in 27 patients (60%), followed by 3 to 6 months duration in 9 patients (20%), 6 to 12 months duration in 7 patients (15.6%) and more than 12 months duration was seen in 2 patients (4.4%). A study done by Chavan et al [12] reported the maximum (40%) number of cases in the age group of 21-40 and most of the patients had disease duration of less than 3 months.
All the patients had multiple lesions and 97.8% of patients gave history of progression of disease and aggravating factors such as cold, stress and trauma seen in 68.9%, 57.8% and 37.8% patients respectively. The mean duration of symptoms in the patients included in the study was 4.58 months. A family history of psoriasis was seen in 13.3% patients. A study by Mehta et al [13] which had 61 patients of psoriasis found that the mean duration of the disease was 1.3 years±2.1 years with a range of 1 month-10 years and they found winter exacerbation in 24(39.3%). A study by Kaur et al [14] reported only 2% positive family history, but another study by Bedi et al [15] reported positive family history in 14% of the patients.
In our study, we found that maximum number of lesions was distributed on the trunk in 86.7% patients followed by lower limbs (62.2%), upper limbs (55.6%), scalp (13.3%). The lesions were present as a combination of scaly papules and plaques arranged symmetrically in 91.1% patients. There is a lot of variation in the most common site of involvement reported. A study by Okhandiar et al [16] found that the extensors (93%) were the most common site of involvement followed by the scalp (88%). Bedi et al [15] in their study found that the most common site of involvement was trunk, followed by trunk, limbs, scalp, face, palms soles and flexures. Kaur et al [14] reported scalp (25%) as the most commonly involved site followed by legs (20.6%) and arms (11.7%).
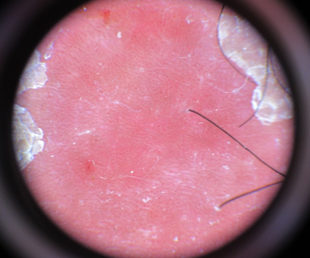
Dermoscopic examination showed dotted vessels in all 45 patients (100%) and additionally red globules were seen in 8 patients (17.8%), the most common pattern of arrangement of vessels was in a regular distribution, seen in 43 patients (95.6%) and were associated with white scales in all (100%) patients, which were diffusely distributed in 93.3% with a light red background in 88.9% and dull red background in 6.7% cases. ([Figure 5])
The dermoscopic finding of our study were comparable to a study by Lallas et al[6] who found that 83 (49%) patients out of 169 had psoriasis and on dermoscopy, dotted vessels were seen in all (100%) cases which were more commonly arranged in a regular distribution (88%) and were associated with white scales (70%) in a diffuse distribution in 45% patients. The combination of specific dermoscopic features such as dotted vessels distributed homogeneously over a light red background in association with diffuse white scales lead to a correct diagnosis of psoriasis with 88% of specificity and 84.9% of sensitivity.
Similar results were obtained in another study by Lallas et al[17] in which dotted vessels were seen in 135 of 139 lesions (97.1%), with regular distribution of vessels in 87.7%. White scales were seen in 64.7%. Scales were diffusely distributed in 44.6%, patchily in 14.4%.
Additionally, a study by Vazquez-Lopez et al [7] had described the presence of “red globules arranged in irregular circles or rings” (red globular rings) as highly specific feature of plaque psoriasis.
HPE of all the biopsy specimens showed Hyperkeratosis, Parakeratosis, Acanthosis, Munro’s microabscess, Hypo granulosis, dilated vessels and perivascular infiltrate. ([Figure 6]) The histopathological features seen in the initial phase of the plaque are edema and capillary dilatation in papillary dermis, lymphocytic infiltrates, slight spongiosis of lower epidermis and absent granular layer; mounds of parakeratosis are formed with neutrophils seen in summit of some of these (early Munro’s microabscesses); neutrophils can form spongiform pustules of Kogoj in upper most portion of spinous layer. In a fully developed plaque, elongation of the dermal papillae and associated dilated, tortuous capillaries are present. Munro microabscesses are seen in the stratum corneum. Regular elongation of the rete ridges, spongiform pustule and acanthosis, diminished to absent granular layer with confluent parakeratosis are typically present. The most important diagnostic features of psoriasis are spongiform pustule and Munro microabscess. [3]
Conclusion
Our study indicates that CPP is more common in young adults and shows a strong male preponderance with flaking of skin being the most symptom at presentation. A combination of specific dermoscopic features such as dotted vessels distributed homogeneously over a light red background in association with diffuse white scales is seen in most cases. Histopathologically, Hyperkeratosis, Parakeratosis, Acanthosis, Munro’s microabscess, Hypo granulosis, dilated vessels and perivascular infiltrate were classically seen. A vast number of studies in different sub-populations of the country with a larger sample size are required to highlight the characteristic epidemiological, clinical dermoscopic and histopathological aspects of CPP.
Conflicts of Interest
None.
Source of Funding
None.
References
- Pavithran K, Karunakaran M, Palit A, Valia R. Disorders of keratinization. IADVL Textbook of Dermatology. 3rd Edn.. 2000;1:1021-56. [Google Scholar]
- Dogra S, Yadav S. Psoriasis in India: Prevalence and pattern. Indian J Dermatol Venereol Leprol. 2010;76(6):595-601. [Google Scholar] [Crossref]
- Mobini N, Toussaint S, Kamino H, DE, RE, BJJ, et al. Non – infectious erythematous papular and squamous disorders. Lever’s histopathology of skin. 9th edn.. 2005. [Google Scholar]
- Lallas A, Zalaudek I, Argenziano G, Longo C, Moscarella E, Di-Lernia V. Dermoscopy in General Dermatology. Clin Dermatol. 2013;31(4):679-94. [Google Scholar]
- Lallas A, Giacomel J, Argenziano G, Garcia-Garcia B, González-Fernández D, Zalaudek I. Dermoscopy in general dermatology: practical tips for the clinician. Br J Dermatol. 2014;170(3):514-26. [Google Scholar] [Crossref]
- Lallas A, Kyrgidis A, Tzellos TG, Apalla Z, Karakyriou E, Karatolias A. Accuracy of dermoscopic criteria for the diagnosis of psoriasis, dermatitis, lichen planus and pityriasis rosea. Br J Dermatol. 2012;166(6):1198-205. [Google Scholar] [Crossref]
- Vazquez-Lopez F, Manjon-Haces J, Maldonado-Seral C, Raya-Aguado C, Pe´rez-Oliva N, Marghoob A. Dermoscopic features of plaque psoriasis and lichen planus: new observations. Venereol Leprol. 2003;207(2):151-6. [Google Scholar] [Crossref]
- Zalaudek I, Argenziano G. Dermoscopy subpatterns of inflammatory skin disorders. Arch Dermatol. 2006;142(6). [Google Scholar] [Crossref]
- Meglio P, Villanova F, Nestle F. Psoriasis. Cold Spring Harb Perspect Med. 2014;4. [Google Scholar] [Crossref]
- Asokan N, Prathap P, Ajithkumar K, Betsy A, Binesh V, Sandhya G. Pattern of skin diseases among patients attending a tertiary care teaching hospital in Kerala. Indian J Dermatol Venereol Leprol. 2009;75(5):517-8. [Google Scholar] [Crossref]
- Dogra A, Arora AK. Nail psoriasis: the journey so far. Indian J Dermatol. 2014;59(4):319-33. [Google Scholar] [Crossref]
- Chavhan S, Mahajan S, Vankudre A. A descriptive study on patients of papulosquamous lesion at tertiary care institute. MVP J Med Sci. 2014;1(1). [Google Scholar]
- Mehta S, Singhal A, Bhattacharya SN. A study of clinicopathological correlation in patients of psoriasis and psoriasiform dermatitis. Indian J Dermatol Venerol Leprol. 2009;75(1). [Google Scholar] [Crossref]
- Kaur I, Handa S, Kumar B. Natural history of psoriasis: A study from Indian subcontinent. J Dermatol. 1997;24(4):230-4. [Google Scholar] [Crossref]
- Bedi TR. Clinical profile of psoriasis in North India. Indian J Dermatol Venerol Leprol. 1995;61(4):202-5. [Google Scholar]
- Okhandiar R, Banerjee B. Psoriasis in the tropics: An epidemiology survey. J Indian Med Assoc. 1963;41:550-6. [Google Scholar]
- Lallas A, Apalla Z, Karteridou A. Dermoscopy for discriminating between pityriasis rubra pilaris and psoriasis. J Dermatol Case Rep. 2013;7(1):20-2. [Google Scholar] [Crossref]